

Diagnostic Performance of Breast Magnetic Resonance Imaging in Non-Calcified Equivocal Breast Findings: Results from a Systematic Review and Meta-Analysis
- PMID: 27482715
- PMCID: PMC4970763
- DOI: 10.1371/journal.pone.0160346
Diagnostic Performance of Breast Magnetic Resonance Imaging in Non-Calcified Equivocal Breast Findings: Results from a Systematic Review and Meta-Analysis
Abstract
Objectives: To evaluate the performance of MRI for diagnosis of breast cancer in non-calcified equivocal breast findings.
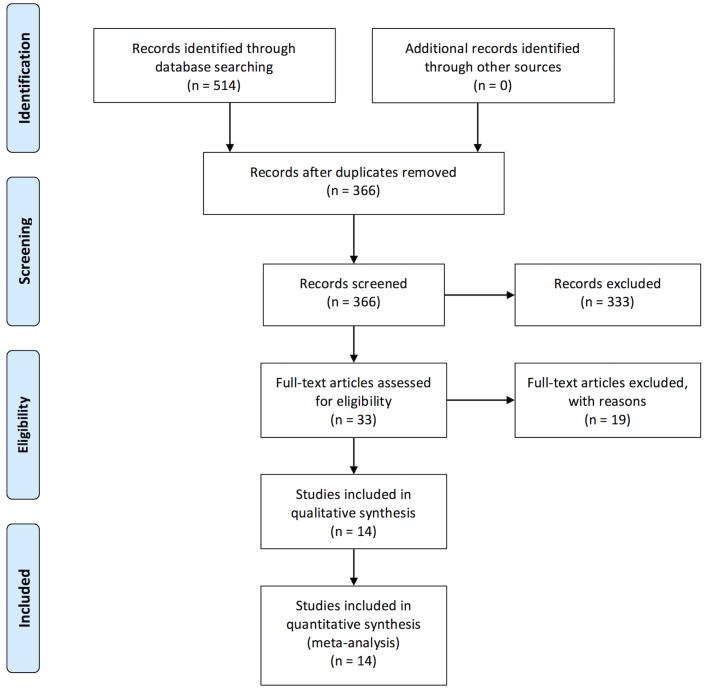
Materials and methods: We performed a systematic review and meta-analysis of peer-reviewed studies in PubMed from 01/01/1986 until 06/15/2015. Eligible were studies applying dynamic contrast-enhanced breast MRI as an adjunct to conventional imaging (mammography, ultrasound) to clarify equivocal findings without microcalcifications. Reference standard for MRI findings had to be established by histopathological sampling or imaging follow-up of at least 12 months. Number of true or false positives and negatives and other characteristics were extracted, and possible bias was determined using the QUADAS-2 applet. Statistical analyses included data pooling and heterogeneity testing.
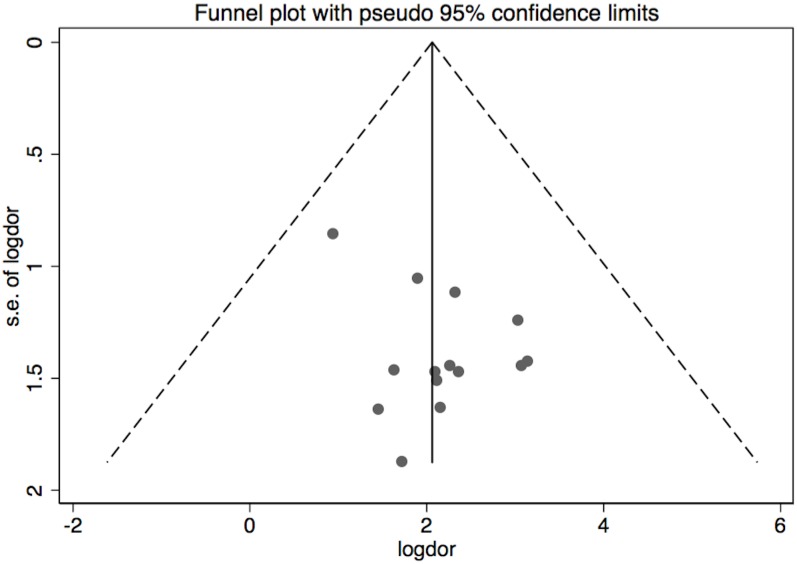
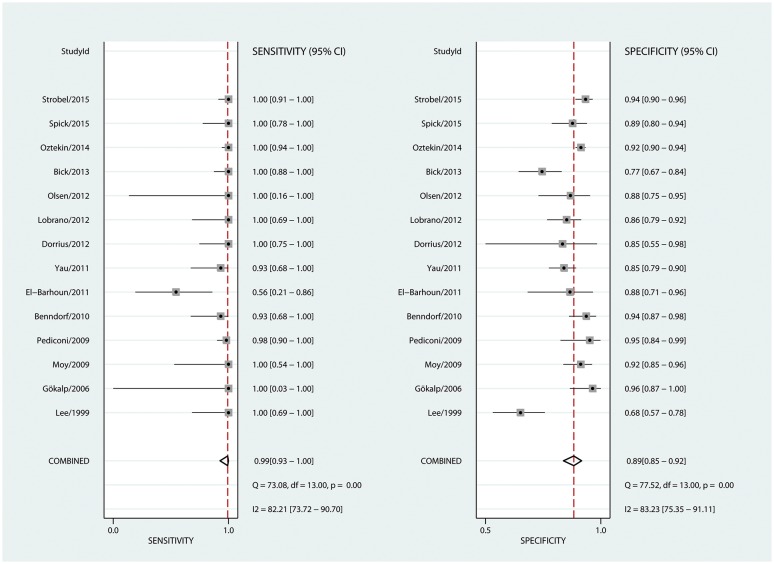
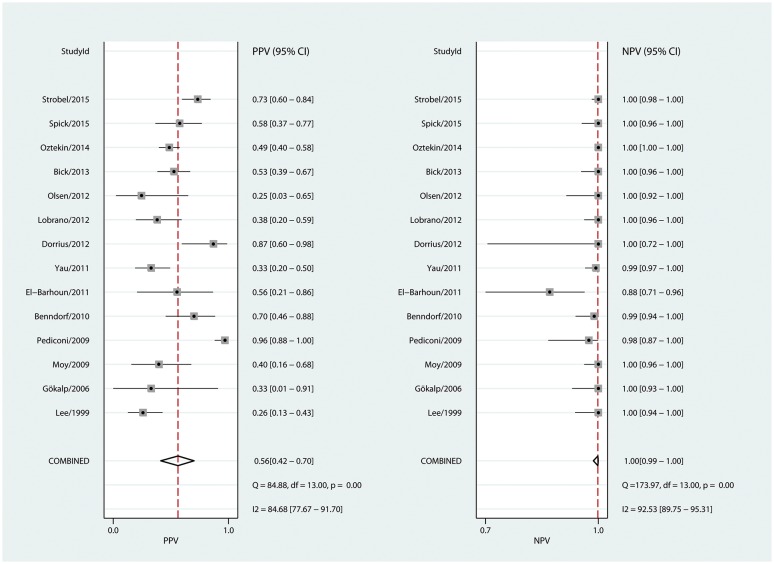
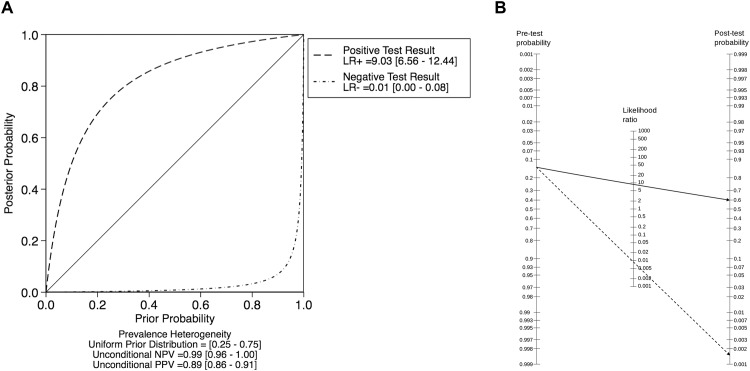
Results: Fourteen out of 514 studies comprising 2,316 lesions met our inclusion criteria. Pooled diagnostic parameters were: sensitivity (99%, 95%-CI: 93-100%), specificity (89%, 95%-CI: 85-92%), PPV (56%, 95%-CI: 42-70%) and NPV (100%, 95%-CI: 99-100%). These estimates displayed significant heterogeneity (P<0.001).
Conclusions: Breast MRI demonstrates an excellent diagnostic performance in case of non-calcified equivocal breast findings detected in conventional imaging. However, considering the substantial heterogeneity with regard to prevalence of malignancy, problem solving criteria need to be better defined.
Conflict of interest statement
Figures
References
-
- Kreienberg R (coordinator). Interdisciplinary German S3 Guidelines for the Diagnosis, Treatment and Follow-up Care of Breast Cancer [Internet]. 2012. Available: www.awmf.org
-
- Early and locally advanced breast cancer: diagnosis and treatment | Guidance and guidelines | NICE [Internet]. [cited 21 Feb 2016]. Available: https://www.nice.org.uk/guidance/cg80
-
- Houssami N, Ciatto S, Macaskill P, Lord SJ, Warren RM, Dixon JM, et al. Accuracy and surgical impact of magnetic resonance imaging in breast cancer staging: systematic review and meta-analysis in detection of multifocal and multicentric cancer. J Clin Oncol Off J Am Soc Clin Oncol. 2008;26: 3248–3258.: 10.1200/JCO.2007.15.2108 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
