

CT in ovarian cancer staging: how to review and report with emphasis on abdominal and pelvic disease for surgical planning
- PMID: 27484100
- PMCID: PMC4971689
- DOI: 10.1186/s40644-016-0076-2
CT in ovarian cancer staging: how to review and report with emphasis on abdominal and pelvic disease for surgical planning
Abstract
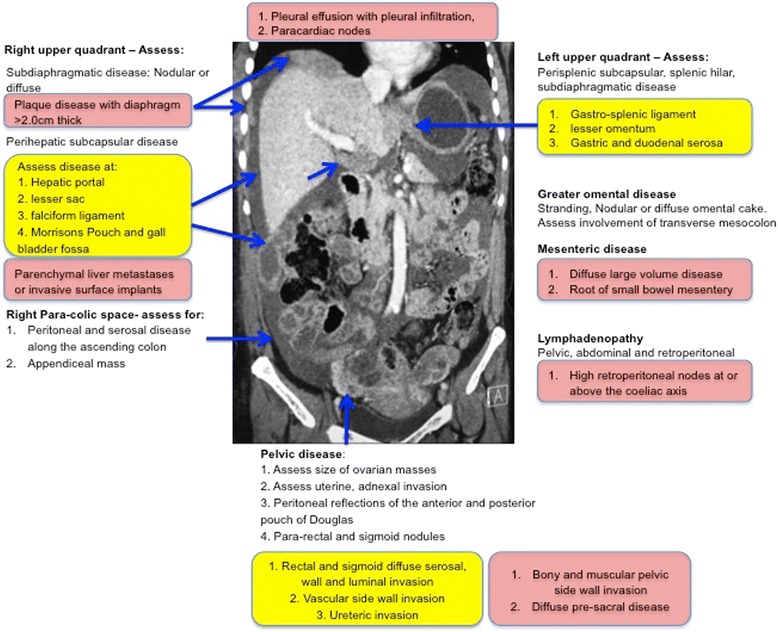
CT of the abdomen and pelvis is the first line imaging modality for staging, selecting treatment options and assessing disease response in ovarian cancer. The staging CT provides disease distribution, disease burden and is the imaging surrogate for surgico-pathological FIGO staging. Optimal cyto-reductive surgery offers patients' the best chance for disease control or cure, but sub-optimal resection confers no advantage over chemotherapy and adversely increases the risk of post surgical complications. Although there is extensive literature comparing performance of CT against laparoscopy and surgery, for the staging abdominal and pelvic CT, there are currently no accepted guidelines for interpretation or routinely used minimum data set templates for reporting these complex CT scans often with extensive radiological findings. This review provides a systematic approach for identifying the important radiological findings and highlighting important sites of disease within the abdomen and pelvis, which may alter or preclude surgery at presentation or after adjuvant chemotherapy. The distribution of sites and volume of disease can be used to categorize patients as suitable, probably suitable or not suitable for optimal cyto-reductive surgery. This categorization can potentially assist oncological surgeons and oncologists as a semi objective assessment tool useful for selecting patient treatment, streamlining multi disciplinary discussion and improving the reproducibility and correlation of CT with surgical findings. The review also highlights sites of disease and complications of ovarian cancer which should be included as part of the radiological report as these may require additional surgical input from non gynaecological surgeons or influence treatment selection.
Keywords: CT; Disease distribution; Ovarian cancer; Surgical resection; Template reporting.
Figures


References
-
- Suidan RS, Ramirez PT, Sarasohn DM, Teitcher JB, Mironov S, Iyer RB, et al. A multicenter prospective trial evaluating the ability of preoperative computed tomography scan and serum CA-125 to predict suboptimal cytoreduction at primary debulking surgery for advanced ovarian, fallopian tube, and peritoneal cancer. Gynecol Oncol. 2014;134(3):455–61. doi: 10.1016/j.ygyno.2014.07.002. - DOI - PMC - PubMed
-
- Hoskins WJ, McGuire WP, Brady MF, Homesley HD, Creasman WT, Berman M, et al. The effect of diameter of largest residual disease on survival after primary cytoreductive surgery in patients with suboptimal residual epithelial ovarian carcinoma. Am J Obstet Gynecol. 1994;170(4):974–9. doi: 10.1016/S0002-9378(94)70090-7. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
