

Association Between Initial Opioid Prescribing Patterns and Subsequent Long-Term Use Among Opioid-Naïve Patients: A Statewide Retrospective Cohort Study
- PMID: 27484682
- PMCID: PMC5215151
- DOI: 10.1007/s11606-016-3810-3
Association Between Initial Opioid Prescribing Patterns and Subsequent Long-Term Use Among Opioid-Naïve Patients: A Statewide Retrospective Cohort Study
Abstract
Background: Long-term efficacy of opioids for non-cancer pain is unproven, but risks argue for cautious prescribing. Few data suggest how long or how much opioid can be prescribed for opioid-naïve patients without inadvertently promoting long-term use.
Objective: To examine the association between initial opioid prescribing patterns and likelihood of long-term use among opioid-naïve patients.
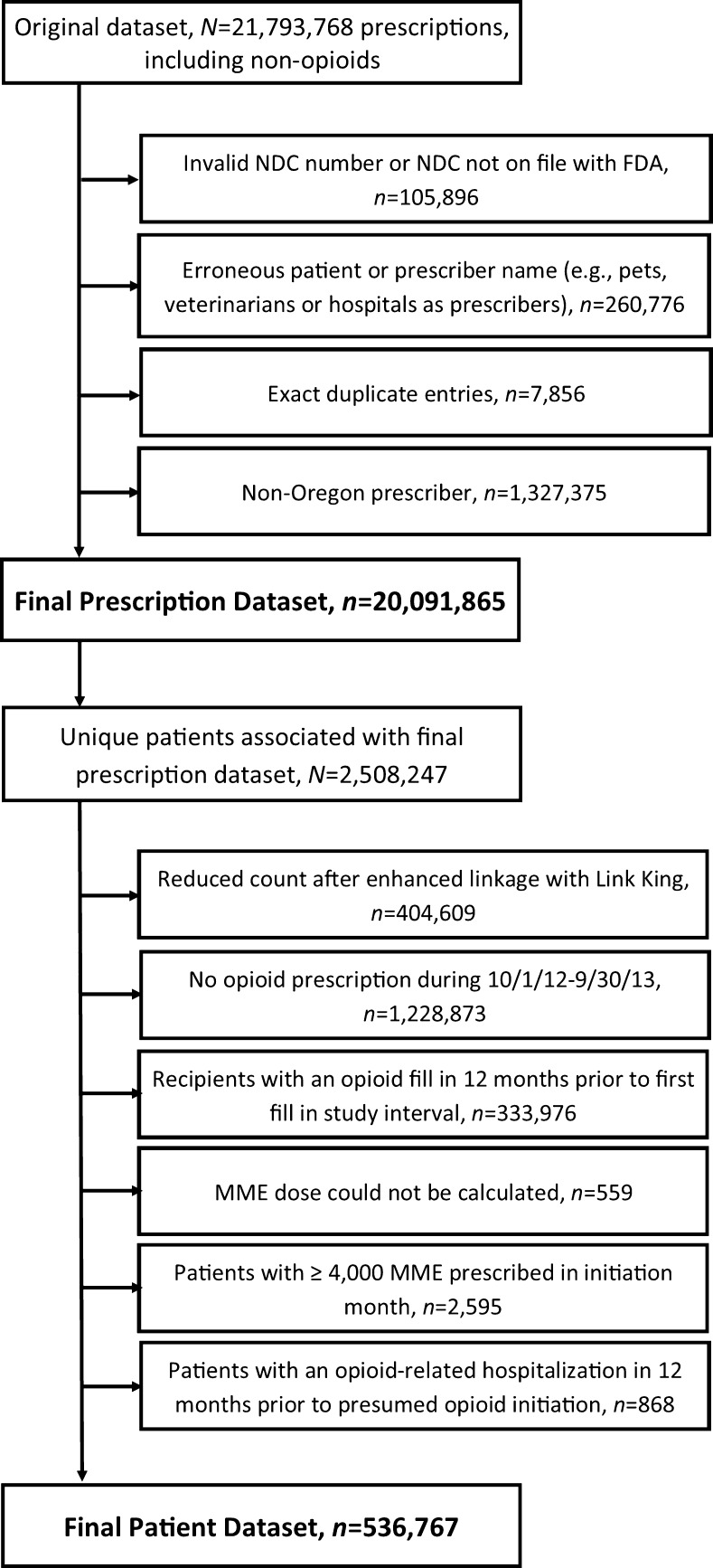
Design: Retrospective cohort study; data from Oregon resident prescriptions linked to death certificates and hospital discharges.
Participants: Patients filling opioid prescriptions between October 1, 2012, and September 30, 2013, with no opioid fills for the previous 365 days. Subgroup analyses examined patients under age 45 who did not die in the follow-up year, excluding most cancer or palliative care patients.
Main measures: Exposure: Numbers of prescription fills and cumulative morphine milligram equivalents (MMEs) dispensed during 30 days following opioid initiation ("initiation month").
Outcome: Proportion of patients with six or more opioid fills during the subsequent year ("long-term users").
Key results: There were 536,767 opioid-naïve patients who filled an opioid prescription. Of these, 26,785 (5.0 %) became long-term users. Numbers of fills and cumulative MMEs during the initiation month were associated with long-term use. Among patients under age 45 using short-acting opioids who did not die in the follow-up year, the adjusted odds ratio (OR) for long-term use among those receiving two fills versus one was 2.25 (95 % CI: 2.17, 2.33). Compared to those who received < 120 total MMEs, those who received between 400 and 799 had an OR of 2.96 (95 % CI: 2.81, 3.11). Patients initiating with long-acting opioids had a higher risk of long-term use than those initiating with short-acting drugs.
Conclusions: Early opioid prescribing patterns are associated with long-term use. While patient characteristics are important, clinicians have greater control over initial prescribing. Our findings may help minimize the risk of inadvertently initiating long-term opioid use.
Keywords: opioid initiation; opioid-naïve; opioids; pain; prescription drug monitoring programs.
Conflict of interest statement
Compliance with Ethical Standards Prior Presentations None Conflict of Interest Richard A. Deyo discloses that he receives royalties from UpToDate for authoring topics on low back pain, and previously received honoraria for board membership at the nonprofit Informed Medical Decisions Foundation. His salary at Oregon Health & Science University is supported in part by an endowment from Kaiser Permanente. He received a financial award from NuVasive as part of a lifetime achievement award from the International Society for the Study of the Lumbar Spine. All other authors declare no conflicts of interest.
Figures
Comment in
-
Opportunities to Improve Decision-Making About Opioid Prescribing.J Gen Intern Med. 2017 Jan;32(1):3-5. doi: 10.1007/s11606-016-3847-3. J Gen Intern Med. 2017. PMID: 27599486 Free PMC article. No abstract available.
-
Among opioid-naive patients receiving opioids, more intensive opioid prescribing in the first month is associated with transition to long-term opioid use.Evid Based Med. 2017 Jun;22(3):112. doi: 10.1136/ebmed-2017-110710. Epub 2017 May 13. Evid Based Med. 2017. PMID: 28501803 No abstract available.
References
-
- Paulozzi LJ, Jones CM, Mack KA, Rudd RA. Vital signs: overdoses of prescription opioid pain relievers, United States, 1999–2008. MMWR Morb Mortal Wkly Rep. 2011;60:1487–92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
