

A co-design process developing heuristics for practitioners providing end of life care for people with dementia
- PMID: 27484683
- PMCID: PMC4969644
- DOI: 10.1186/s12904-016-0146-z
A co-design process developing heuristics for practitioners providing end of life care for people with dementia
Erratum in
-
Erratum to: A co-design process developing heuristics for practitioners providing end of life care for people with dementia.BMC Palliat Care. 2016 Aug 18;15(1):77. doi: 10.1186/s12904-016-0148-x. BMC Palliat Care. 2016. PMID: 27538391 Free PMC article. No abstract available.
Abstract
Background: The end of life for someone with dementia can present many challenges for practitioners; such as, providing care if there are swallowing difficulties. This study aimed to develop a toolkit of heuristics (rules-of-thumb) to aid practitioners making end-of-life care decisions for people with dementia.
Methods: An iterative co-design approach was adopted using a literature review and qualitative methods, including; 1) qualitative interviews and focus groups with family carers and 2) focus groups with health and care professionals. Family carers were recruited from a national charity, purposively sampling those with experience of end-of-life care for a person with dementia. Health and care professionals were purposively sampled to include a broad range of expertise including; general practitioners, palliative care specialists, and geriatricians. A co-design group was established consisting of health and social care experts and family carers, to synthesise the findings from the qualitative work and produce a toolkit of heuristics to be tested in practice.
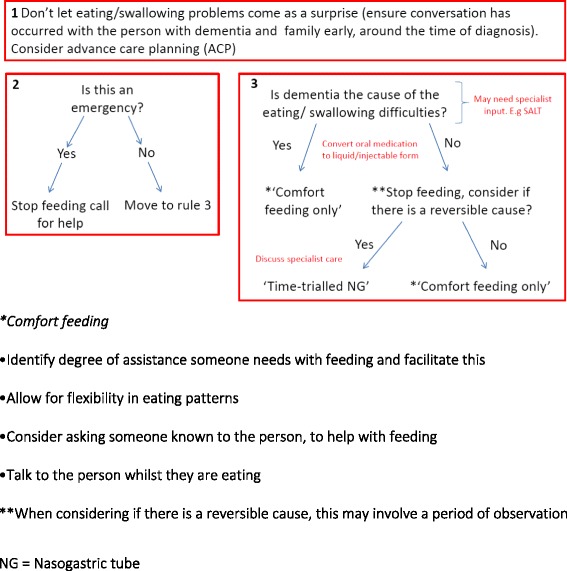
Results: Four broad areas were identified as requiring complex decisions at the end of life; 1) eating/swallowing difficulties, 2) agitation/restlessness, 3) ending life-sustaining treatment, and 4) providing "routine care" at the end of life. Each topic became a heuristic consisting of rules arranged into flowcharts. Eating/swallowing difficulties have three rules; ensuring eating/swallowing difficulties do not come as a surprise, considering if the situation is an emergency, and considering 'comfort feeding' only versus time-trialled artificial feeding. Agitation/restlessness encourages a holistic approach, considering the environment, physical causes, and the carer's wellbeing. Ending life-sustaining treatment supports practitioners through a process of considering the benefits of treatment versus quality-of-life and comfort. Finally, a heuristic on providing routine care such as bathing, prompts practitioners to consider adapting the delivery of care, in order to promote comfort and dignity at the end of life.
Conclusions: The heuristics are easy to use and remember, offering a novel approach to decision making for dementia end-of-life care. They have the potential to be used alongside existing end-of-life care recommendations, adding more readily available practical assistance. This is the first study to synthesise experience and existing evidence into easy-to-use heuristics for dementia end-of-life care.
Keywords: Co-design; Dementia; End-of-life care; Palliative care; Qualitative research.
Figures





References
-
- Alzheimer’s Disease International: Dementia and Risk Reduction: An analysis of protective and modifiable factors. In. London; 2014.
-
- Matthews FE, Arthur A, Barnes LE, Bond J, Jagger C, Robinson L, Brayne C. A two-decade comparison of prevalence of dementia in individuals aged 65 years and older from three geographical areas of England: results of the Cognitive Function and Ageing Study I and II. Lancet. 2013;382(9902):1405–1412. doi: 10.1016/S0140-6736(13)61570-6. - DOI - PMC - PubMed
-
- Alzheimer’s Disease International: World Alzheimer Report 2015: The Global Impact of Dementia: An analysis of prevalence, incidence, cost and trends. In. Edited by International AsD. London; 2015.
-
- Chan KY, Wang W, Wu JJ, Liu L, Theodoratou E, Car J, Middleton L, Russ TC, Deary IJ, Campbell H, et al. Epidemiology of Alzheimer’s disease and other forms of dementia in China, 1990–2010: a systematic review and analysis. Lancet. 2013;381(9882):2016–2023. doi: 10.1016/S0140-6736(13)60221-4. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
