

Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 1. Disease Burden and Principles of Care
- PMID: 27486151
- PMCID: PMC4994789
- DOI: 10.1177/0706743716659416
Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 1. Disease Burden and Principles of Care
Abstract
Background: The Canadian Network for Mood and Anxiety Treatments (CANMAT) conducted a revision of the 2009 guidelines by updating the evidence and recommendations. The scope of the 2016 guidelines remains the management of major depressive disorder (MDD) in adults, with a target audience of psychiatrists and other mental health professionals.
Methods: Using the question-answer format, we conducted a systematic literature search focusing on systematic reviews and meta-analyses. Evidence was graded using CANMAT-defined criteria for level of evidence. Recommendations for lines of treatment were based on the quality of evidence and clinical expert consensus. This section is the first of six guidelines articles.
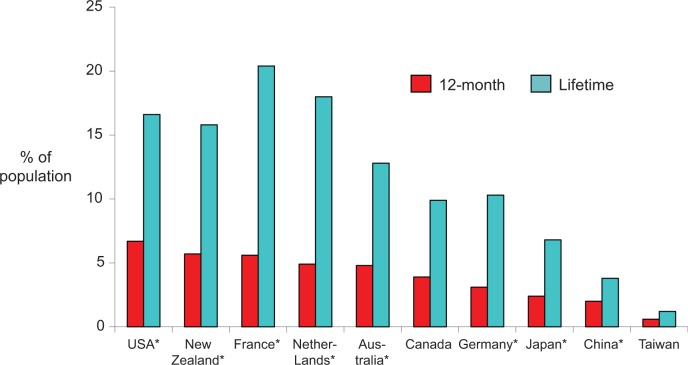
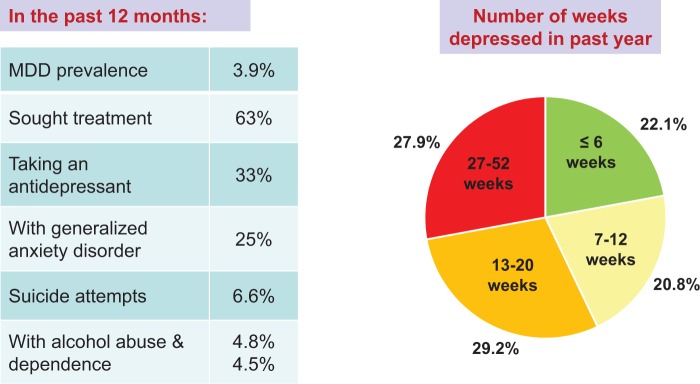
Results: In Canada, the annual and lifetime prevalence of MDD was 4.7% and 11.3%, respectively. MDD represents the second leading cause of global disability, with high occupational and economic impact mainly attributable to indirect costs. DSM-5 criteria for depressive disorders remain relatively unchanged, but other clinical dimensions (sleep, cognition, physical symptoms) may have implications for depression management. e-Mental health is increasingly used to support clinical and self-management of MDD. In the 2-phase (acute and maintenance) treatment model, specific goals address symptom remission, functional recovery, improved quality of life, and prevention of recurrence.
Conclusions: The burden attributed to MDD remains high, whether from individual distress, functional and relationship impairment, reduced quality of life, or societal economic cost. Applying core principles of care, including comprehensive assessment, therapeutic alliance, support of self-management, evidence-informed treatment, and measurement-based care, will optimize clinical, quality of life, and functional outcomes in MDD.
Keywords: clinical assessment; clinical practice guidelines; depressive disorders; diagnosis; evidence-based medicine; major depressive disorder; meta-analysis; phenomenology; systematic reviews.
© The Author(s) 2016.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RWL has received honoraria for ad hoc speaking or advising/consulting or received research funds from Asia-Pacific Economic Cooperation, AstraZeneca, Brain Canada, Bristol-Myers Squibb, Canadian Institutes of Health Research, Canadian Depression Research and Intervention Network, Canadian Network for Mood and Anxiety Treatments, Canadian Psychiatric Association, Coast Capital Savings, Johnson & Johnson, Lundbeck, Lundbeck Institute, Medscape, Pfizer, St. Jude Medical, Takeda, University Health Network Foundation, and Vancouver Coastal Health Research Institute. DM has received honoraria for ad hoc speaking or advising/consulting or received research funds from Allergan, Bristol-Myers Squibb, Lundbeck, Janssen-Ortho, Otsuka, Pfizer, Shire, and Sunovion. JLW has no disclosures. MWE has no disclosures. TK has received speaker and/or advisory honoraria from AstraZeneca, Bristol-Myers Squibb, Eli Lilly Canada, Lundbeck, Lundbeck-Otsuka, Janssen-Ortho, Pfizer, and Sunovion. EEM has received advisory honoraria from Lundbeck. JS has no disclosures. WYS has received honoraria for ad hoc speaking or advising/consulting or research funds from AstraZeneca, Bristol-Myers Squibb, Canadian Psychiatric Association, Eli Lilly, Forrest Laboratories, Lundbeck, Ortho-Janssen, Pfizer, and Sunovion. SHK has received honoraria for ad hoc speaking or advising/consulting or research funds from Allergan, Brain Canada, Bristol-Myers Squibb, Canadian Institutes of Health Research, Janssen, Lundbeck, Ontario Brain Institute, Pfizer, St. Jude Medical, Servier, and Sunovion. GMM has been on advisory board or speaker for Janssen, Lilly, Lundbeck, and Pfizer. RVM has received speaker and consultant honoraria or research funds from Allergan, Bristol-Myers Squibb, Canadian Institutes of Health Research, Canadian Network for Mood and Anxiety Treatments, Canadian Psychiatric Association, Eli Lilly, Johnson & Johnson, Lallemand, Lundbeck, Merck, Ontario Brain Institute, Ontario Mental Health Foundation, Otsuka, Paladin, Pfizer, Queen’s University, Sunovion, Takeda, the University Health Network Foundation, and Valeant. SVP has been a consultant to Bristol Myers Squibb, Lundbeck, and Takeda; has had a research contract with Assurex; and has equity in Mensante. AVR has received speaker and consultant honoraria or research funds from Bristol-Myers Squibb, Canadian Depression Research and Intervention Network, Canadian Foundation for Innovation and the Ministry of Economic Development and Innovation, Canadian Institutes of Health Research, Grand Challenges Canada, Janssen, Lundbeck, Ontario Mental Health Foundation, Pfizer, and Sunovion.
Figures
References
-
- Kennedy SH, Lam RW, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) clinical guidelines for the management of major depressive disorder in adults. Introduction. J Affect Disord. 2009;11(Suppl 1):S1–S2. - PubMed
-
- Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) collaborative update of CANMAT guidelines for the management of patients with bipolar disorder: update 2013. Bipolar Disord. 2013;15:1–44. - PubMed
-
- American Psychiatric Association (APA). Diagnostic and statistical manual of mental disorders. 5th ed Arlington (VA; ): American Psychiatric Association; 2013.
-
- World Health Organization. The ICD-10 classification of mental and behavioural disorders: diagnostic criteria for research. Geneva (Switzerland): World Health Organization; 1992.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
