

Beyond Contact Tracing: Community-Based Early Detection for Ebola Response
- PMID: 27486552
- PMCID: PMC4946441
- DOI: 10.1371/currents.outbreaks.322427f4c3cc2b9c1a5b3395e7d20894
Beyond Contact Tracing: Community-Based Early Detection for Ebola Response
Abstract
Introduction: The 2014 Ebola outbreak in West Africa raised many questions about the control of infectious disease in an increasingly connected global society. Limited availability of contact information made contact tracing diffcult or impractical in combating the outbreak.
Methods: We consider the development of multi-scale public health strategies that act on individual and community levels. We simulate policies for community-level response aimed at early screening all members of a community, as well as travel restrictions to prevent inter-community transmission.
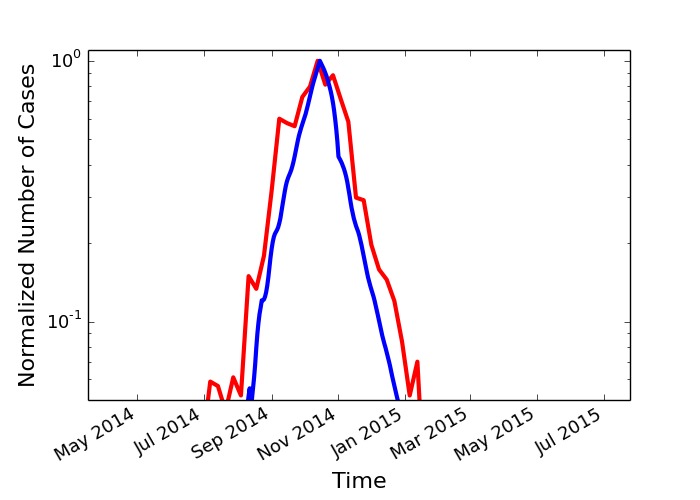
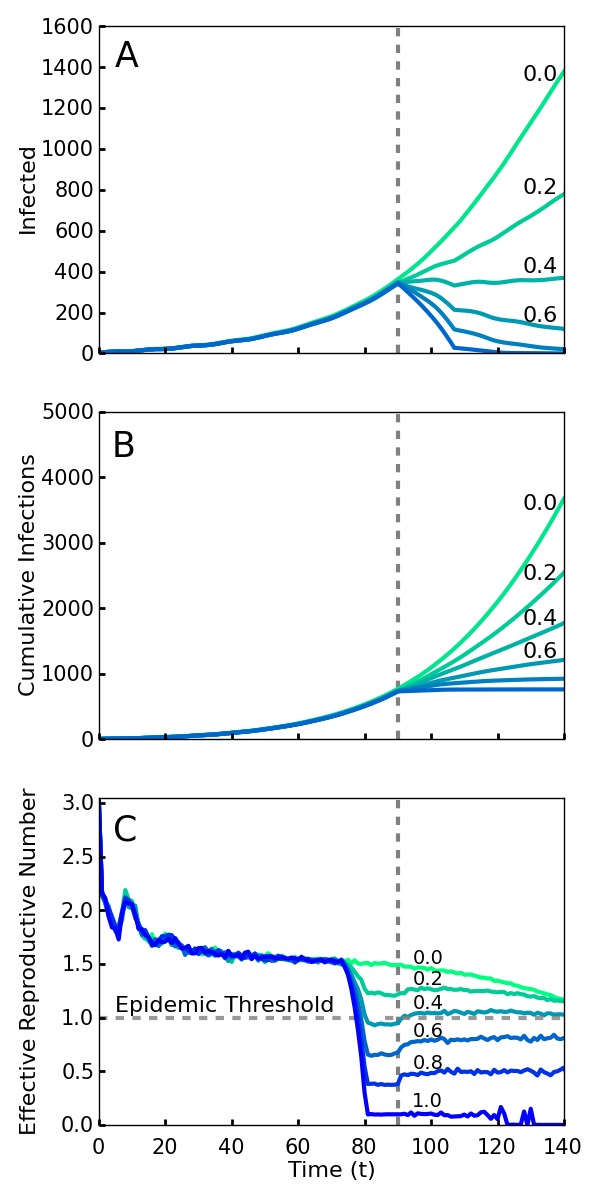
Results: Our analysis shows the policies to be effective even at a relatively low level of compliance and for a variety of local and long range contact transmission networks. In our simulations, 40% of individuals conforming to these policies is enough to stop the outbreak. Simulations with a 50% compliance rate are consistent with the case counts in Liberia during the period of rapid decline after mid September, 2014. We also find the travel restriction to be effective at reducing the risks associated with compliance substantially below the 40% level, shortening the outbreak and enabling efforts to be focused on affected areas.
Discussion: Our results suggest that the multi-scale approach can be used to further evolve public health strategy for defeating emerging epidemics.
Figures

References
-
- World Health Organization (WHO). Contact tracing during an outbreak of ebola virus disease. WHO. Published September 2015. Accessed February 1, 2016.
-
- World Health Organization (WHO). Frequently asked questions on ebola virus disease. WHO. Published August 2014.
-
- Tsimring LS, Huerta R. Modeling of contact tracing in social networks. Physica A: Statistical Mechanics and its Applications. 2003;325(1-2):33-39.
LinkOut - more resources
Full Text Sources
Other Literature Sources
