

Effectiveness of sulphonylureas in the therapy of diabetes mellitus type 2 patients: an observational cohort study
- PMID: 27486568
- PMCID: PMC4969981
- DOI: 10.1186/s40200-016-0251-9
Effectiveness of sulphonylureas in the therapy of diabetes mellitus type 2 patients: an observational cohort study
Abstract
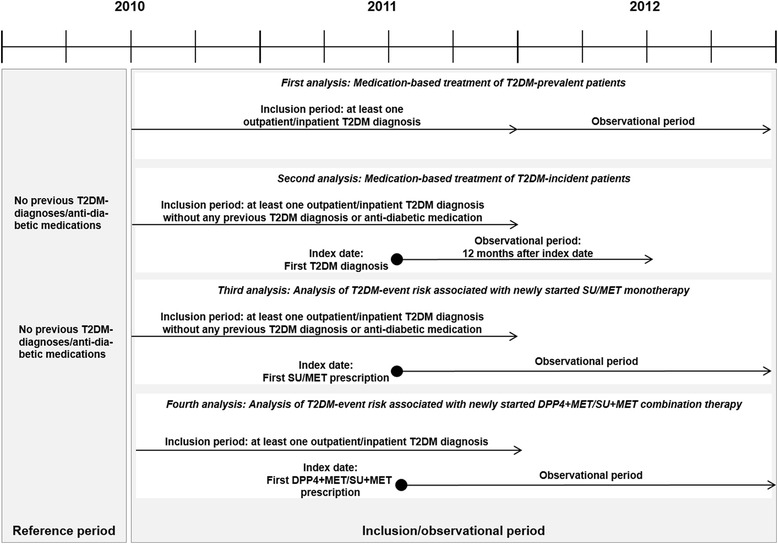
Background: We compared all-cause mortality, major macrovascular events (MACE) and diabetes-related hospitalizations in T2DM-incident patients newly treated with metformin (MET) versus sulphonylureas (SU) monotherapy and in T2DM-prevalent patients newly treated with MET+SU versus MET+DPP4-inhibitor combination therapy.
Methods: We analysed anonymized data obtained from a German health fund. Patients were included when they had started MET versus SU therapy or MET+SU versus MET+DPP4 therapy between 01/07/2010 and 31/12/2011. Observation started with the first MET/SU prescription or the first prescription of the second agent of a MET+SU/MET+DPP4 combination therapy. Follow-up time lasted until the end of data availability (a minimum of 12 months), death or therapy discontinuation.
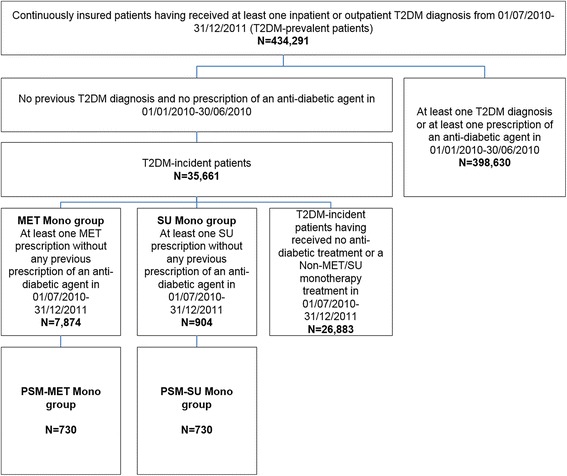
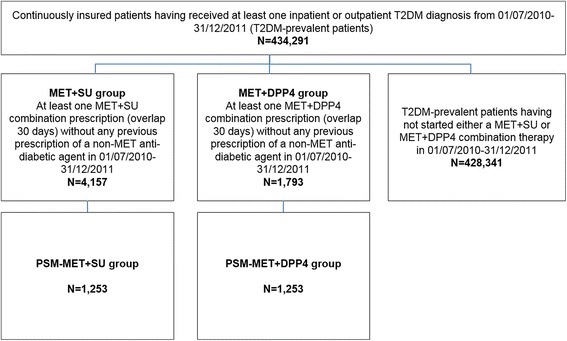
Results: In total, 434,291 T2DM-prevalent and 35,661 T2DM-incident patients were identified. Of the identified T2DM-incident patients, 904/7,874 started SU/MET monotherapy, respectively, with a mean age of 70.1/61.4 years (54.6/50.3 % female; Charlson Comorbidity Index (CCI) 1.4/2.2; 933/7,350 observed SU/MET patient years). 4,157/1,793 SU+MET/DPP4+MET therapy starters had a mean age of 68.1/62.2 years (53.4/50.8 % female; CCI 2.8/2.6; 4,556/1,752 observed SU+MET/ DPP4+MET patient years). In a propensity score matched (PSM) comparison, the HRs (95 % CIs) associated with SU monotherapy compared to MET monotherapy exposure were 1.4 (0.9-2.3) for mortality, 1.4 (0.9-2.2) for MACE, 4.1 (1.5-10.9) for T2DM hospitalizations and 1.6 (1.2-2.3) for composite event risk. In a multivariable Cox regression model, SU monotherapy was associated with higher mortality (aHR 2.0; 1.5-2.6), higher MACE (aHR 1.3; 1.0-1.7) and higher T2DM hospitalizations (aHR 2.8; 1.8-4.4), which corresponded with a higher composite event risk (aHR 1.8; 1.5-2.1). No significant differences in event rates were observed in the PSM comparison between DPP4+MET/SU+MET combination therapy starters and in the multivariable Cox regression analysis.
Conclusions: Our results show that SU monotherapy may be associated with increased mortality, MACE and T2DM hospitalizations, compared to MET monotherapy. When considering SU therapy, the associated cardiovascular risk should also be taken into account.
Keywords: Antidiabetic therapy; Macrovascular event risk; Mortality risk for type 2 diabetes mellitus patients; Sulphonylureas; T2DM-related hospitalizations; Type 2 diabetes mellitus.
Figures
Similar articles
-
Important differences in the durability of glycaemic response among second-line treatment options when added to metformin in type 2 diabetes: a retrospective cohort study.Ann Med. 2016;48(4):224-34. doi: 10.3109/07853890.2016.1157263. Epub 2016 Mar 16. Ann Med. 2016. PMID: 26982210
-
Comparison of diabetes-associated secondary healthcare utilization between alternative oral antihyperglycaemic dual therapy combinations with metformin in patients with type 2 diabetes: an observational cohort study.Diabetes Obes Metab. 2015 Jun;17(6):573-580. doi: 10.1111/dom.12458. Epub 2015 Apr 6. Diabetes Obes Metab. 2015. PMID: 25735201
-
Real-world antidiabetic drug use and fracture risk in 12,277 patients with type 2 diabetes mellitus: a nested case-control study.Osteoporos Int. 2018 Sep;29(9):2079-2086. doi: 10.1007/s00198-018-4581-y. Epub 2018 Jun 2. Osteoporos Int. 2018. PMID: 29860664
-
Repaglinide : a pharmacoeconomic review of its use in type 2 diabetes mellitus.Pharmacoeconomics. 2004;22(6):389-411. doi: 10.2165/00019053-200422060-00005. Pharmacoeconomics. 2004. PMID: 15099124 Review.
-
Oral antidiabetic agents: current role in type 2 diabetes mellitus.Drugs. 2005;65(3):385-411. doi: 10.2165/00003495-200565030-00005. Drugs. 2005. PMID: 15669880 Review.
Cited by
-
The Infamous, Famous Sulfonylureas and Cardiovascular Safety: Much Ado About Nothing?Curr Diab Rep. 2017 Oct 23;17(12):124. doi: 10.1007/s11892-017-0954-4. Curr Diab Rep. 2017. PMID: 29063276 Review.
-
Associations between multimorbidity, all-cause mortality and glycaemia in people with type 2 diabetes: A systematic review.PLoS One. 2018 Dec 26;13(12):e0209585. doi: 10.1371/journal.pone.0209585. eCollection 2018. PLoS One. 2018. PMID: 30586451 Free PMC article.
-
Impaired fasting glucose and sulfonylureas increased the risk of major cardiovascular events in patients with inflammatory arthritis.Diabetol Metab Syndr. 2025 Apr 19;17(1):132. doi: 10.1186/s13098-025-01689-6. Diabetol Metab Syndr. 2025. PMID: 40251690 Free PMC article.
References
-
- Robert Koch-Institut (RKI). Daten und Fakten: Ergebnisse der Studie “Gesundheit in Deutschland aktuell 2009” - Beiträge zur GBE [cited 2016 Mar 4]. Available from: URL:https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichter....
-
- Wilke T, Mueller S, Groth A, Fuchs A, Seitz L, Kienhöfer J, et al. Treatment-dependent and treatment-independent risk factors associated with the risk of diabetes-related events: a retrospective analysis based on 229,042 patients with type 2 diabetes mellitus. Cardiovasc Diabetol. 2015;14:14. doi: 10.1186/s12933-015-0179-2. - DOI - PMC - PubMed
-
- Chang HY, Weiner JP, Richards TM, Bleich SN, Segal JB. Validating the adapted Diabetes Complications Severity Index in claims data. Am J Manag Care. 2012;18:721–6. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
