

Altered Treg and cytokine responses in RSV-infected infants
- PMID: 27486703
- PMCID: PMC6215710
- DOI: 10.1038/pr.2016.130
Altered Treg and cytokine responses in RSV-infected infants
Abstract
Background: Respiratory syncytial virus (RSV) is the leading cause of bronchiolitis and pneumonia in children under 1 y of age in the USA. The host immune response is believed to contribute to RSV-induced disease. We hypothesize that severe RSV infection in infants is mediated by insufficient regulation of the host immune response of regulatory T cells (Tregs) resulting in immunopathology.
Methods: Blood and nasal aspirates from 23 RSV-infected and 17 control infants under 1 y of age were collected. Treg frequencies were determined by flow cytometry from peripheral blood mononuclear cells. Analysis of 24 cytokines was measured by multiplex assay on nasal aspirates.
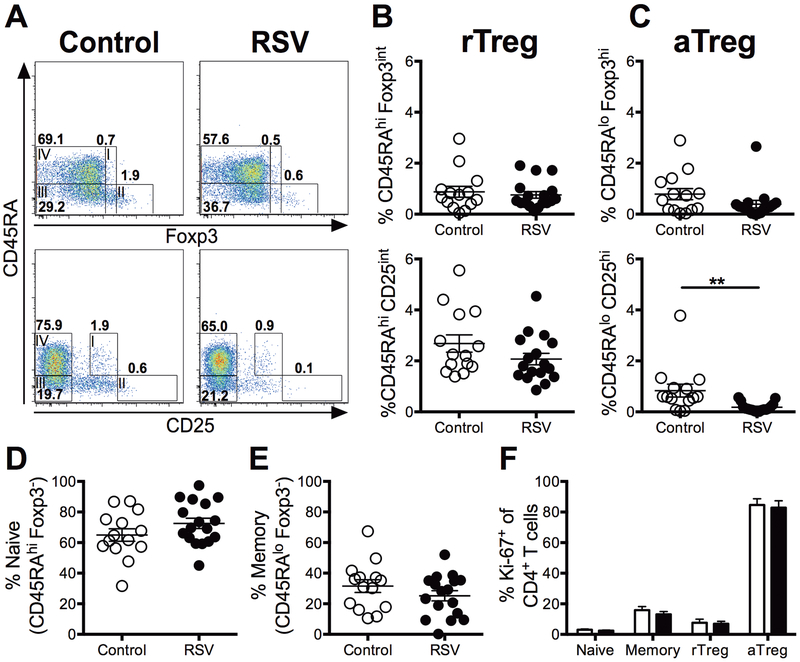
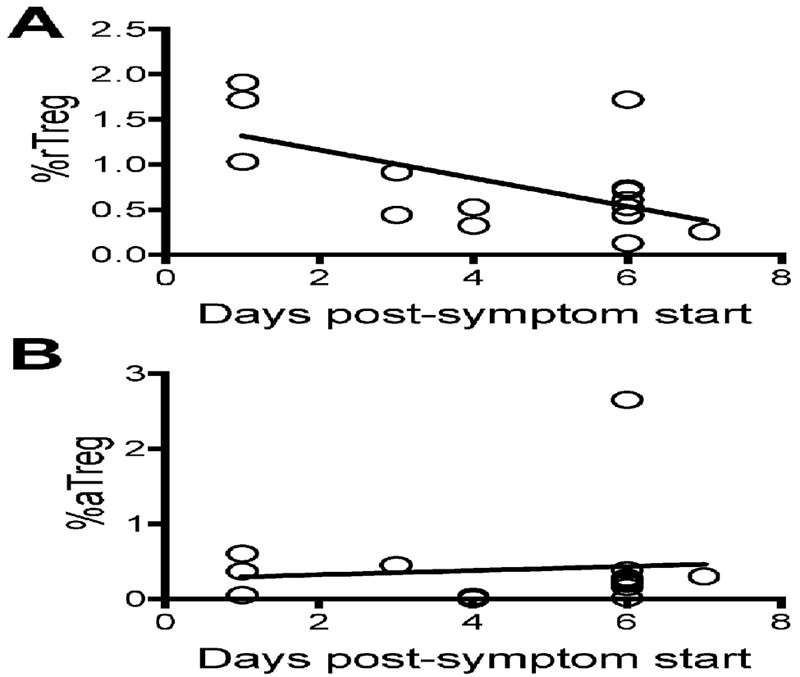
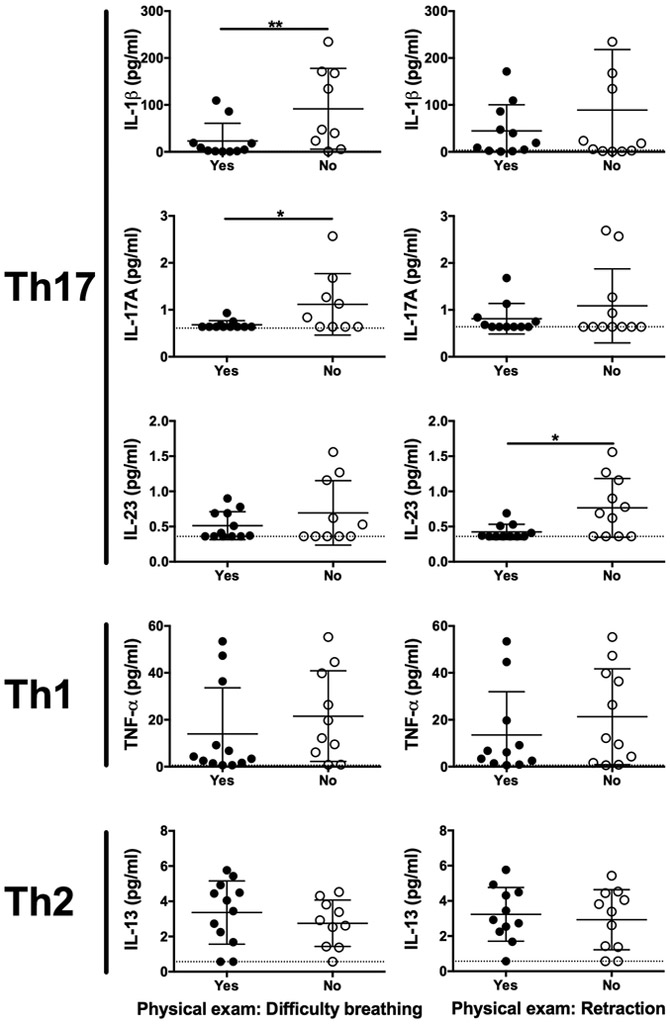
Results: We demonstrate that the frequency of activated Tregs is significantly reduced in the peripheral blood of RSV-infected infants compared with age-matched controls. Surprisingly, T helper (Th)17 related cytokines including interleukin (IL)-1β, IL-17A, and IL-23 were associated with a reduction in clinical symptoms of respiratory distress. In addition, the amount of IL-33 protein in nasal washes, a cytokine important in maintaining Treg homeostasis in mucosal tissues, was decreased in RSV-infected children.
Conclusion: These results suggest that decreased Treg numbers and an inability to properly control the host inflammatory response results in severe RSV infection.
Conflict of interest statement
The authors would like to note that there are no conflicts of interest to declare.
Figures
References
-
- Glezen WP, Taber LH, Frank AL, Kasel JA Risk of primary infection and reinfection with respiratory syncytial virus. Am J Dis Child 1986;140:543–546. - PubMed
-
- Rivera CA, Gomez RS, Diaz RA, et al. Novel therapies and vaccines against the human respiratory syncytial virus. Expert Opin Investig Drugs 2015:1–18. - PubMed
-
- Johnson S, Oliver C, Prince GA, et al. Development of a humanized monoclonal antibody (MEDI-493) with potent in vitro and in vivo activity against respiratory syncytial virus. J Infect Dis 1997;176:1215–1224. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
