

Practice Patterns and Outcomes Associated With Use of Anticoagulation Among Patients With Atrial Fibrillation During Sepsis
- PMID: 27487456
- PMCID: PMC5810586
- DOI: 10.1001/jamacardio.2016.2181
Practice Patterns and Outcomes Associated With Use of Anticoagulation Among Patients With Atrial Fibrillation During Sepsis
Abstract
Importance: Atrial fibrillation (AF) during sepsis is associated with an increased risk of ischemic stroke during hospitalization, but risks and benefits associated with anticoagulation for AF during sepsis are unclear.
Objective: To determine clinician practice patterns and patient risk of stroke and bleeding associated with use of anticoagulation for AF during sepsis.
Design, setting, and participants: A retrospective cohort study using enhanced administrative claims data from approximately 20% of patients hospitalized in the United States July 1, 2010, to June 30, 2013, examined patients with AF during sepsis who did not have additional indications for therapeutic anticoagulation. Propensity score and instrumental variable analyses were used to evaluate risks of in-hospital stroke and bleeding associated with anticoagulation during sepsis.
Exposures: Parenteral anticoagulants administered in doses greater than those used for prophylaxis of venous thromboembolism.
Main outcomes and measures: Ischemic stroke and clinically significant bleeding events during hospitalization.
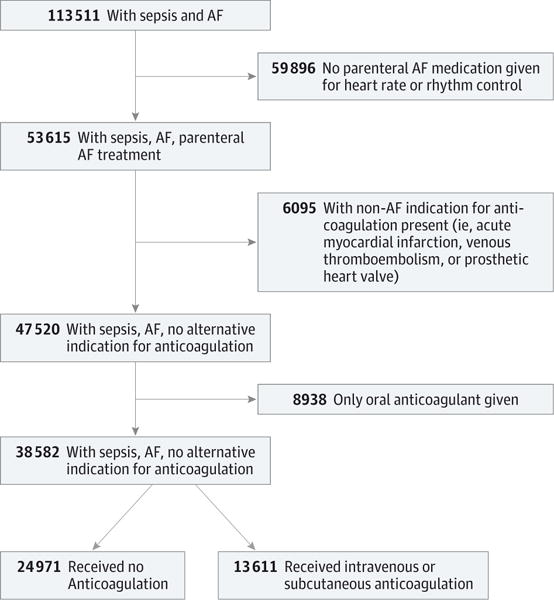
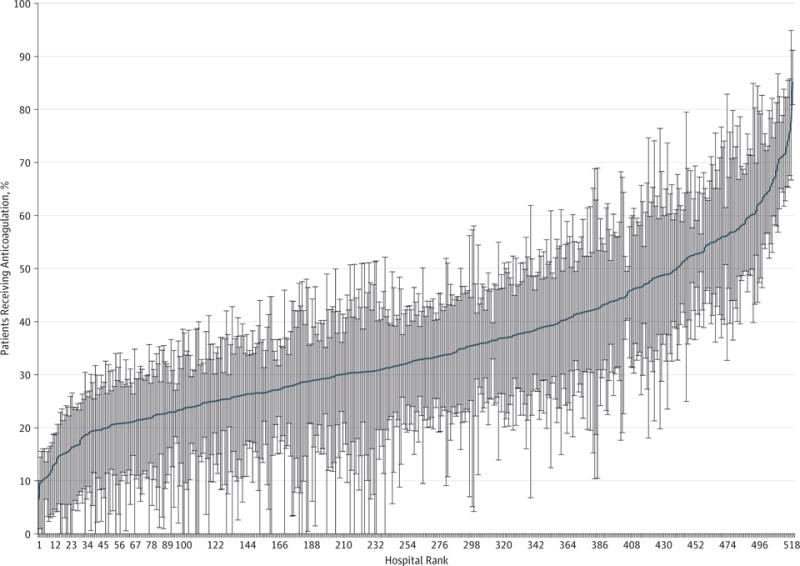
Results: Of 113 511 patients hospitalized with AF and sepsis, 38 582 were included in our primary analysis (18 976 men and 19 606 women; mean [SD] age, 74.9 [11.7] years). A total of 13 611 patients (35.3%) received parenteral anticoagulants, while 24 971 (64.7%) did not. Hospital utilization rates of parenteral anticoagulants for AF during sepsis varied (median, 33%; 25th-75th percentile, 25%-43%). CHA2DS2VASc scores (congestive heart failure, hypertension, age ≥75 years [doubled], type 1 or type 2 diabetes, stroke or transient ischemic attack or thromboembolism [doubled], vascular disease [prior myocardial infarction, peripheral artery disease, or aortic plaque], age 65-75 years, sex category [female]) poorly discriminated the risk of ischemic stroke during sepsis (C statistic, 0.526). Among 27 010 propensity score-matched patients, rates of in-hospital ischemic stroke events did not differ significantly between patients who did (174 of 13 505 [1.3%]) and did not (185 of 13 505 [1.4%]) receive parenteral anticoagulation (relative risk [RR], 0.94; 95% CI, 0.77-1.15). Clinically significant bleeding occurred more often among patients who received parenteral anticoagulation (1163 of 13 505 [8.6%]) than patients who did not receive parenteral anticoagulation (979 of 13 505 [7.2%]; RR, 1.21; 95% CI, 1.10-1.32). Risk of ischemic stroke associated with parenteral anticoagulation did not differ significantly between patients with preexisting (RR, 1.12; 95% CI, 0.86-1.44) or newly diagnosed AF (RR, 0.85; 95% CI 0.57-1.27; P = .31 for interaction). Results were robust to multiple sensitivity analyses, including hospital utilization rates of parenteral anticoagulation for AF as an instrument for anticoagulation exposure (RR for stroke, 1.08; 95% CI, 0.62-1.90; RR for bleeding, 1.23; 95% CI, 0.88-1.72).
Conclusions and relevance: Among patients with AF during sepsis, parenteral anticoagulation was not associated with reduced risk of ischemic stroke and was associated with higher bleeding rates.
Conflict of interest statement
Figures
Comment in
-
Exploring the Potential Benefits and Risks of Anticoagulation for Atrial Fibrillation During Hospitalization for Sepsis.JAMA Cardiol. 2016 Sep 1;1(6):690-1. doi: 10.1001/jamacardio.2016.2193. JAMA Cardiol. 2016. PMID: 27487233 No abstract available.
References
-
- Torio CM, Andrews RM. Healthcare Cost and Utilization Project Statistical Brief #160. Rockville, MD: Agency for Healthcare Research and Quality; National inpatient hospital costs: the most expensive conditions by payer, 2011. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb160.pdf. Published August 2013. Accessed June 17, 2015. - PubMed
-
- Annane D, Sébille V, Duboc D, et al. Incidence and prognosis of sustained arrhythmias in critically ill patients. Am J Respir Crit Care Med. 2008;178(1):20–25. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
