

Pregnancy Following Bariatric Surgery-Medical Complications and Management
- PMID: 27488114
- PMCID: PMC5018021
- DOI: 10.1007/s11695-016-2294-x
Pregnancy Following Bariatric Surgery-Medical Complications and Management
Abstract
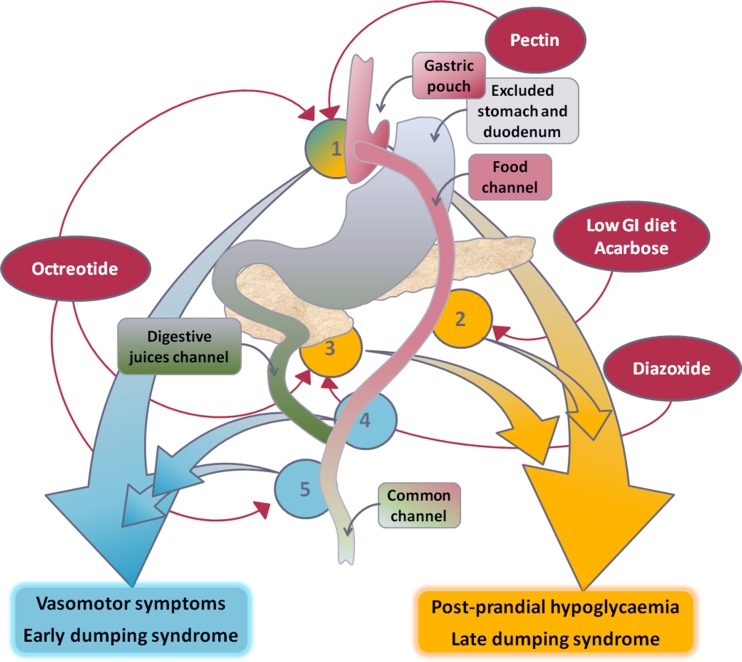
Bariatric surgery is most commonly carried out in women of childbearing age. Whilst fertility rates are improved, pregnancy following bariatric surgery poses several challenges. Whilst rates of many adverse maternal and foetal outcomes in obese women are reduced after bariatric surgery, pregnancy is best avoided for 12-24 months to reduce the potential risk of intrauterine growth retardation. Dumping syndromes are common after bariatric surgery and can present diagnostic and therapeutic challenges in pregnancy. Early dumping occurs due to osmotic fluid shifts resulting from rapid gastrointestinal food transit, whilst late dumping is characterized by a hyperinsulinemic response to rapid absorption of simple carbohydrates. Dietary measures are the mainstay of management of dumping syndromes but pharmacotherapy may sometimes become necessary. Acarbose is the least hazardous pharmacological option for the management of postprandial hypoglycemia in pregnancy. Nutrient deficiencies may vary depending on the type of surgery; it is important to optimize the nutritional status of women prior to and during pregnancy. Dietary management should include adequate protein and calorie intake and supplementation of vitamins and micronutrients. A high clinical index of suspicion is required for early diagnosis of surgical complications of prior weight loss procedures during pregnancy, including small bowel obstruction, internal hernias, gastric band erosion or migration and cholelithiasis.
Keywords: Bariatric surgery; Dumping syndrome; Obesity; Postabsorptive hypoglycemia; Pregnancy.
Conflict of interest statement
The authors declare that they have no conflicts of interest. Informed consent was obtained from the patient in the case report. This article does not contain any studies with human participants or animals performed by any of the authors.
Figures
Comment in
-
Pregnancy Following Bariatric Surgery-Medical Complications and Management.Obes Surg. 2016 Nov;26(11):2785. doi: 10.1007/s11695-016-2362-2. Obes Surg. 2016. PMID: 27573511 No abstract available.
-
Response to Letter Regarding 'Pregnancy Following Bariatric Surgery-Medical Complications and Management'.Obes Surg. 2016 Dec;26(12):3008. doi: 10.1007/s11695-016-2363-1. Obes Surg. 2016. PMID: 27654904 No abstract available.
References
-
- World Obesity. Global overweight & obesity: prevalence of overweight and obesity in adults around the globe. London: World Obesity; 2015 [cited 2015 09 June]; Available from: http://www.worldobesity.org/aboutobesity/resources/obesity-data-portal/r....
-
- Centre for Maternal and Child Enquiries . Maternal obesity in the UK: findings from a national project. London: CMACE; 2010.
-
- Modder J, Fitzsimons, KJ. CMACE/RCOG joint guideline: management of women with obesity in pregnancy. London: Centre for Maternal and Child Enquiries and the Royal College of Obstetricians and Gynaecologists, 2010.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
