

A process evaluation of a cluster randomised trial to reduce potentially inappropriate prescribing in older people in primary care (OPTI-SCRIPT study)
- PMID: 27488272
- PMCID: PMC4973100
- DOI: 10.1186/s13063-016-1513-z
A process evaluation of a cluster randomised trial to reduce potentially inappropriate prescribing in older people in primary care (OPTI-SCRIPT study)
Abstract
Background: The OPTI-SCRIPT cluster randomised controlled trial (RCT) found that a three-phase multifaceted intervention including academic detailing with a pharmacist, GP-led medicines reviews, supported by web-based pharmaceutical treatment algorithms, and tailored patient information leaflets, was effective in reducing potentially inappropriate prescribing (PIP) in Irish primary care. We report a process evaluation exploring the implementation of the intervention, the experiences of those participating in the study and lessons for future implementation.
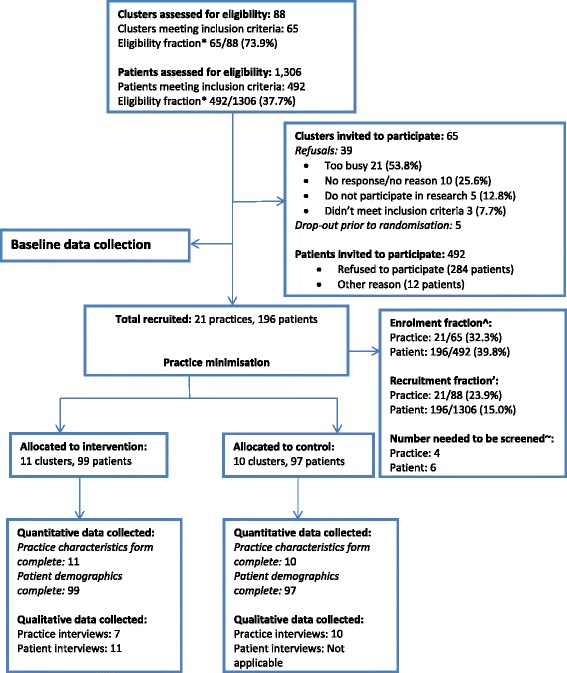
Methods: The OPTI-SCRIPT trial included 21 GP practices and 196 patients. The process evaluation used mixed methods. Quantitative data were collected from all GP practices and semi-structured interviews were conducted with GPs from intervention and control groups, and a purposive sample of patients from the intervention group. All interviews were transcribed verbatim and analysed using a thematic analysis.
Results: Despite receiving a standardised academic detailing session, intervention delivery varied among GP practices. Just over 70 % of practices completed medicines review as recommended with the patient present. Only single-handed practices conducted reviews without patients present, highlighting the influence of practice characteristics and resources on variation. Medications were more likely to be completely stopped or switched to another more appropriate medication when reviews were conducted with patients present. The patient information leaflets were not used by any of the intervention practices. Both GP (32 %) and patient (40 %) recruitment rates were modest. For those who did participate, overall, the experience was positively viewed, with GPs and patients referring to the value of medication reviews to improve prescribing and reduce unnecessary medications. Lack of time in busy GP practices and remuneration were identified as organisational barriers to future implementation.
Conclusions: The OPTI-SCRIPT intervention was positively viewed by both GPs and patients, both of whom valued the study's objectives. Patient information leaflets were not a successful component of the intervention. Academic detailing and medication reviews are important components in changing PIP, and having patients present during the review process seems to be a more effective approach for decreasing PIP.
Trial registration: Current controlled trials ISRCTN41694007 . Registered on 21 March 2012.
Keywords: Cluster randomised controlled trial; Potentially inappropriate prescribing; Primary care; Process evaluation.
Figures



References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
