

Comparison of 10 single and stepped methods to identify frail older persons in primary care: diagnostic and prognostic accuracy
- PMID: 27488562
- PMCID: PMC4973108
- DOI: 10.1186/s12875-016-0487-y
Comparison of 10 single and stepped methods to identify frail older persons in primary care: diagnostic and prognostic accuracy
Abstract
Background: Many instruments have been developed to identify frail older adults in primary care. A direct comparison of the accuracy and prevalence of identification methods is rare and most studies ignore the stepped selection typically employed in routine care practice. Also it is unclear whether the various methods select persons with different characteristics. We aimed to estimate the accuracy of 10 single and stepped methods to identify frailty in older adults and to predict adverse health outcomes. In addition, the methods were compared on their prevalence of the identified frail persons and on the characteristics of persons identified.
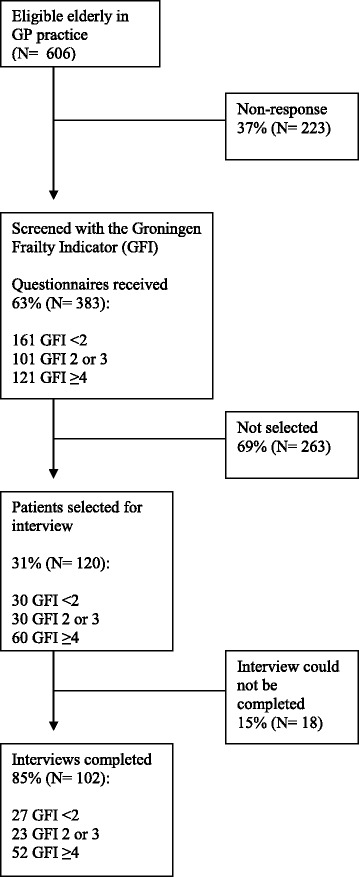
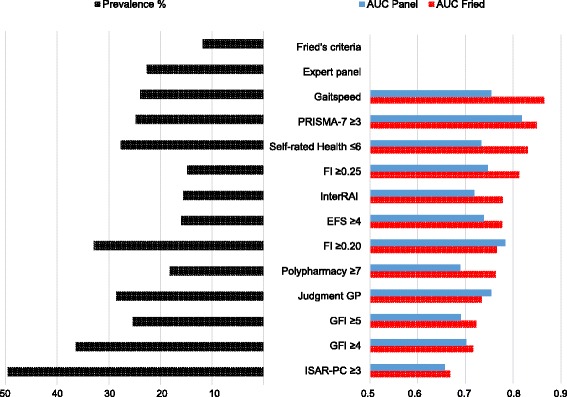
Methods: The Groningen Frailty Indicator (GFI), the PRISMA-7, polypharmacy, the clinical judgment of the general practitioner (GP), the self-rated health of the older adult, the Edmonton Frail Scale (EFS), the Identification Seniors At Risk Primary Care (ISAR PC), the Frailty Index (FI), the InterRAI screener and gait speed were compared to three measures: two reference standards (the clinical judgment of a multidisciplinary expert panel and Fried's frailty criteria) and 6-years mortality or long term care admission. Data were used from the Dutch Identification of Frail Elderly Study, consisting of 102 people aged 65 and over from a primary care practice in Amsterdam. Frail older adults were oversampled. The accuracy of each instrument and several stepped strategies was estimated by calculating the area under the ROC-curve.
Results: Prevalence rates of frailty ranged from 14.8 to 52.9 %. The accuracy for recommended cut off values ranged from poor (AUC = 0.556 ISAR-PC) to good (AUC = 0.865 gait speed). PRISMA-7 performed best over two reference standards, GP predicted adversities best. Stepped strategies resulted in lower prevalence rates and accuracy. Persons selected by the different instruments varied greatly in age, IADL dependency, receiving homecare and mood.
Conclusion: We found huge differences between methods to identify frail persons in prevalence, accuracy and in characteristics of persons they select. A necessary next step is to find out which frail persons can benefit from intervention before case finding programs are implemented. Further evidence is needed to guide this emerging clinical field.
Keywords: Accuracy; Frail elderly; Frailty identification; Older people; Primary care; Stepped approach.
Figures




References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
