

Meta-analysis of colorectal cancer follow-up after potentially curative resection
- PMID: 27488593
- PMCID: PMC5031212
- DOI: 10.1002/bjs.10233
Meta-analysis of colorectal cancer follow-up after potentially curative resection
Abstract
Background: After potentially curative resection of primary colorectal cancer, patients may be monitored by measurement of carcinoembryonic antigen and/or CT to detect asymptomatic metastatic disease earlier.
Methods: A systematic review and meta-analysis was conducted to find evidence for the clinical effectiveness of monitoring in advancing the diagnosis of recurrence and its effect on survival. MEDLINE (Ovid), Embase, the Cochrane Library, Web of Science and other databases were searched for randomized comparisons of increased intensity monitoring compared with a contemporary standard policy after resection of primary colorectal cancer.
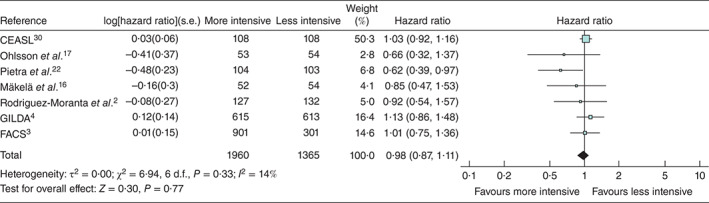
Results: There were 16 randomized comparisons, 11 with published survival data. More intensive monitoring advanced the diagnosis of recurrence by a median of 10 (i.q.r. 5-24) months. In ten of 11 studies the authors reported no demonstrable difference in overall survival. Seven RCTs, published from 1995 to 2016, randomly assigned 3325 patients to a monitoring protocol made more intensive by introducing new methods or increasing the frequency of existing follow-up protocols versus less invasive monitoring. No detectable difference in overall survival was associated with more intensive monitoring protocols (hazard ratio 0·98, 95 per cent c.i. 0·87 to 1·11).
Conclusion: Based on pooled data from randomized trials published from 1995 to 2016, the anticipated survival benefit from surgical treatment resulting from earlier detection of metastases has not been achieved.
© 2016 The Authors. BJS published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures



References
-
- Rodriguez-Moranta F, Saló J, Arcusa A, Boadas J, Piñol V, Bessa Xet al. Postoperative surveillance in patients with colorectal cancer who have undergone curative resection: a prospective, multicenter, randomized, controlled trial. J Clin Oncol 2006; 24: 386–393. - PubMed
-
- Primrose JN, Perera R, Gray A, Rose P, Fuller A, Corkhill Aet al. FACS Trial Investigators. Effect of 3 to 5 years of scheduled CEA and CT follow-up to detect recurrence of colorectal cancer: the FACS randomized clinical trial. JAMA 2014; 311: 263–270. - PubMed
-
- Rosati G, Ambrosini G, Barni S, Andreoni B, Corradini G, Luchena Get al. ; GILDA working group. A randomized trial of intensive versus minimal surveillance of patients with resected Dukes B2-C colorectal carcinoma. Ann Oncol 2016; 27: 274–280. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
