

Incident parkinsonism in older adults without Parkinson disease
- PMID: 27488597
- PMCID: PMC5027813
- DOI: 10.1212/WNL.0000000000003059
Incident parkinsonism in older adults without Parkinson disease
Abstract
Objective: To determine the incidence of parkinsonism in community-dwelling older adults without Parkinson disease.
Methods: Four parkinsonian signs were assessed with a modified motor portion of the Unified Parkinson's Disease Rating Scale in 2,001 older adults without parkinsonism. We used Cox proportional hazards models to determine the associations of age and sex with incident parkinsonism (2 or more signs). We calculated the number of events per 1,000 person-years of observation in 3 age strata. Next, we investigated several potential risk factors for incident parkinsonism. Then, we examined longitudinal progression of parkinsonism using discrete-time multistate Markov models.
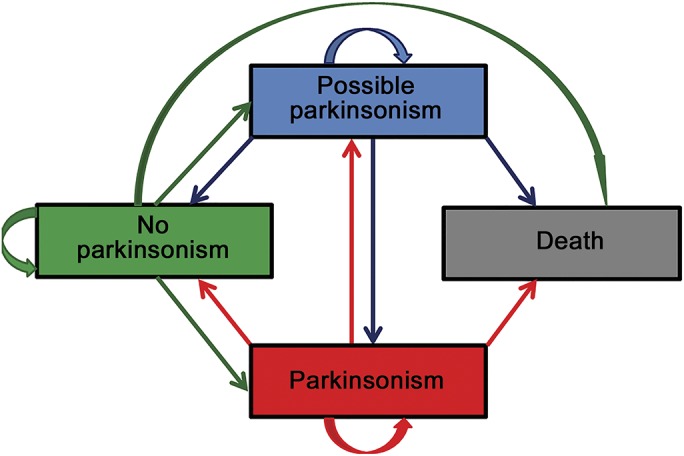
Results: Average age at baseline was 76.8 years (SD 7.62 years). During an average of 5 years of follow-up, 964/2,001 (48.2%) developed parkinsonism. Age (hazard ratio [HR] 1.09, 95% confidence interval [CI] 1.08-1.10) but not male sex (HR 1.06, 95% CI 0.91-1.23) was associated with incident parkinsonism. The incidence of parkinsonism per 1,000 person-years of follow-up was 36.0 for adults <75 years of age, 94.8 for those 75-84, and 160.5 for those 85 years or older. Depressive symptoms, neuroticism, urinary incontinence, sleep complaints, and chronic health conditions were associated with incident parkinsonism. Secondary analyses suggest that risk factors are linked with incident parkinsonism via early motor signs of parkinsonism and cognitive function. Transition modeling suggests that while parkinsonism may fluctuate, it is progressive in most older adults and its risk factors increase the odds of its progression.
Conclusions: Parkinsonism is common in older adults and increases with age. Identifying modifiable risk factors may decrease the magnitude of this growing public health problem.
© 2016 American Academy of Neurology.
Figures
Comment in
-
Letter re: Incident parkinsonism in older adults without Parkinson disease.Neurology. 2017 Feb 28;88(9):919. doi: 10.1212/WNL.0000000000003671. Neurology. 2017. PMID: 28242850 No abstract available.
-
Author response: Incident parkinsonism in older adults without Parkinson disease.Neurology. 2017 Feb 28;88(9):919-920. doi: 10.1212/WNL.0000000000003672. Neurology. 2017. PMID: 28242851 Free PMC article. No abstract available.
-
Letter re: Incident parkinsonism in older adults without Parkinson disease.Neurology. 2017 Feb 28;88(9):920. doi: 10.1212/WNL.0000000000003673. Neurology. 2017. PMID: 28242852 No abstract available.
-
Author response: Incident parkinsonism in older adults without Parkinson disease.Neurology. 2017 Feb 28;88(9):920. doi: 10.1212/WNL.0000000000003674. Neurology. 2017. PMID: 28242853 Free PMC article. No abstract available.
References
-
- Louis ED, Bennett DA. Mild parkinsonian signs: an overview of an emerging concept. Mov Disord 2007;22:1681–1688. - PubMed
-
- Bennett DA, Shannon KM, Beckett LA, Goetz CG, Wilson RS. Metric properties of nurses' ratings of parkinsonian signs with a modified Unified Parkinson's Disease Rating Scale. Neurology 1997;49:1580–1587. - PubMed
MeSH terms
Grants and funding
- U01 AG046152/AG/NIA NIH HHS/United States
- R01 NS078009/NS/NINDS NIH HHS/United States
- U01 AG032984/AG/NIA NIH HHS/United States
- U18 NS082140/NS/NINDS NIH HHS/United States
- P20 MD006886/MD/NIMHD NIH HHS/United States
- R01 AG017917/AG/NIA NIH HHS/United States
- R01 AG043379/AG/NIA NIH HHS/United States
- R01 AG033678/AG/NIA NIH HHS/United States
- R01 AG038651/AG/NIA NIH HHS/United States
- R01 AG022018/AG/NIA NIH HHS/United States
- R01 AG034374/AG/NIA NIH HHS/United States
- R21 NS089854/NS/NINDS NIH HHS/United States
- U01 AG046161/AG/NIA NIH HHS/United States
- R01 AG040039/AG/NIA NIH HHS/United States
- R01 AG033570/AG/NIA NIH HHS/United States
- R01 AG015819/AG/NIA NIH HHS/United States
- R01 AG047976/AG/NIA NIH HHS/United States
- R01 AG042210/AG/NIA NIH HHS/United States
- RF1 AG015819/AG/NIA NIH HHS/United States
- K08 AG034290/AG/NIA NIH HHS/United States
- K01 AG050823/AG/NIA NIH HHS/United States
- R01 AG036042/AG/NIA NIH HHS/United States
- P30 AG010161/AG/NIA NIH HHS/United States
- R01 AG033193/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources