

Why is malaria associated with poverty? Findings from a cohort study in rural Uganda
- PMID: 27488674
- PMCID: PMC4972958
- DOI: 10.1186/s40249-016-0164-3
Why is malaria associated with poverty? Findings from a cohort study in rural Uganda
Abstract
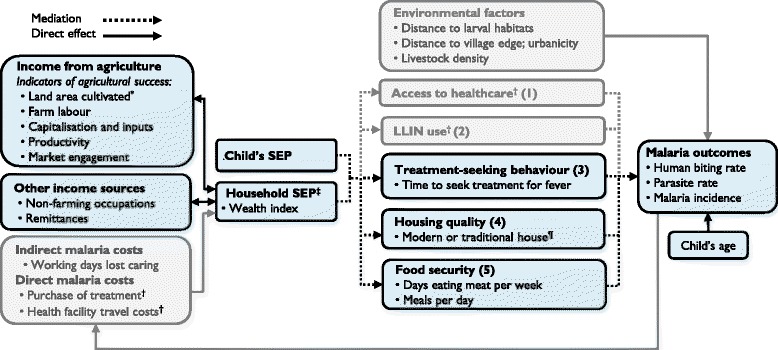
Background: Malaria control and sustainable development are linked, but implementation of 'multisectoral' intervention is restricted by a limited understanding of the causal pathways between poverty and malaria. We investigated the relationships between socioeconomic position (SEP), potential determinants of SEP, and malaria in Nagongera, rural Uganda.
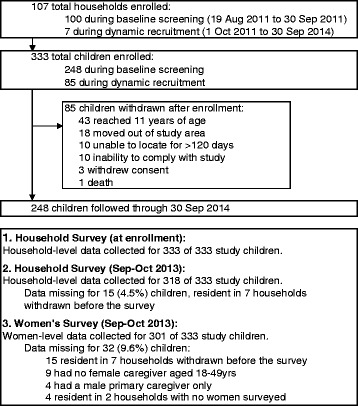
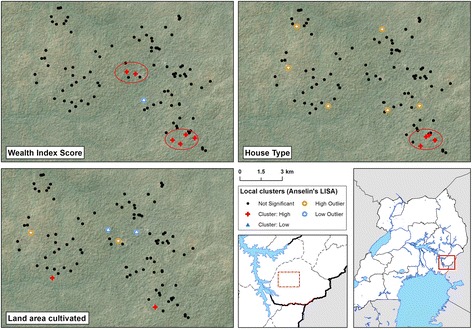
Methods: Socioeconomic information was collected for 318 children aged six months to 10 years living in 100 households, who were followed for up to 36 months. Mosquito density was recorded using monthly light trap collections. Parasite prevalence was measured routinely every three months and malaria incidence determined by passive case detection. First, we evaluated the association between success in smallholder agriculture (the primary livelihood source) and SEP. Second, we explored socioeconomic risk factors for human biting rate (HBR), parasite prevalence and incidence of clinical malaria, and spatial clustering of socioeconomic variables. Third, we investigated the role of selected factors in mediating the association between SEP and malaria.
Results: Relative agricultural success was associated with higher SEP. In turn, high SEP was associated with lower HBR (highest versus lowest wealth index tertile: Incidence Rate Ratio 0.71, 95 % confidence intervals (CI) 0.54-0.93, P = 0.01) and lower odds of malaria infection in children (highest versus lowest wealth index tertile: adjusted Odds Ratio 0.52, 95 % CI 0.35-0.78, P = 0.001), but SEP was not associated with clinical malaria incidence. Mediation analysis suggested that part of the total effect of SEP on malaria infection risk was explained by house type (24.9 %, 95 % CI 15.8-58.6 %) and food security (18.6 %, 95 % CI 11.6-48.3 %); however, the assumptions of the mediation analysis may not have been fully met.
Conclusion: Housing improvements and agricultural development interventions to reduce poverty merit further investigation as multisectoral interventions against malaria. Further interdisplinary research is needed to understand fully the complex pathways between poverty and malaria and to develop strategies for sustainable malaria control.
Keywords: Development; Housing; Malaria; Poverty; Socioeconomic; Uganda; Wealth index.
Figures
References
-
- WHO . World Malaria Report. Geneva: World Health Organization; 2015.
-
- Bhatt S, Weiss DJ, Cameron E, Bisanzio D, Mappin B, Dalrymple U, Battle KE, Moyes CL, Henry A, Eckhoff PA, Wenger EA, Briët O, Penny MA, Smith TA, Bennett A, Yukich J, Eisele TP, Griffin JT, Fergus CA, Lynch M, Lindgren F, Cohen JM, Murray CL, Smith DL, Hay SI, Cibulskis RE, Gething PW. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature. 2015;526:207–11. doi: 10.1038/nature15535. - DOI - PMC - PubMed
-
- Tusting LS, Willey B, Lucas H, Thompson J, Kafy HT, Smith R, Lindsay SW. Socioeconomic development as an intervention against malaria: a systematic review and meta-analysis. Lancet. 2013;382(9895):834. - PubMed
-
- Bruce-Chwatt L, de Zulueta J. The rise and fall of malaria in Europe. London: Oxford University Press; 1980.
-
- RBM/UNDP . Multisectoral Action Framework for Malaria. Geneva: Roll Back Malaria/United Nations Development Programme; 2013.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
