

Review
doi: 10.1016/j.jcot.2016.06.002.
Epub 2016 Jun 28.
Scaffold-free, stem cell-based cartilage repair
Affiliations
- PMID: 27489410
- PMCID: PMC4949412
- DOI: 10.1016/j.jcot.2016.06.002
Item in Clipboard
Review
Scaffold-free, stem cell-based cartilage repair
J Clin Orthop Trauma.
2016 Jul-Sep.
Abstract
Various approaches to treat articular cartilage have been widely investigated due to its poor intrinsic healing capacity. Stem cell-based therapy could be a promising approach as an alternative to chondrocyte-based therapy and some of these therapies have been already applied in clinical condition. This review discusses the current development of stem cell-based therapies in cartilage repair, specifically focusing on scaffold-free approaches.
Keywords: Cartilage repair; Mesenchymal stem cell; Scaffold free; Stem cell-based therapy.
Figures
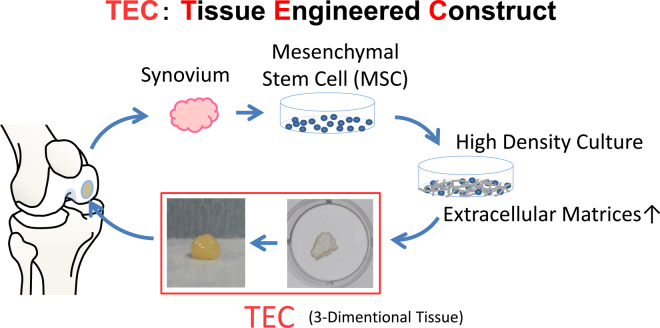
Schematic representation of the TEC-mediated cartilage repair.
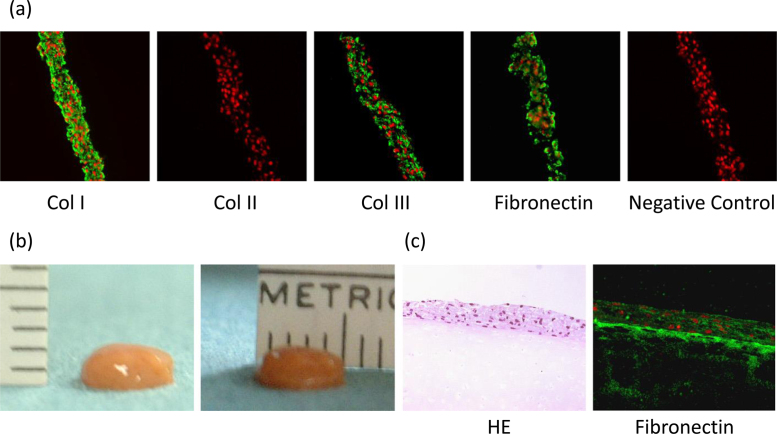
Development of the tissue-engineered construct. (a) Immunohistochemical analysis of the basic TEC stained with type I collagen (Col I), type II collagen (Col II), type III collagen (Col III), fibronectin, and negative IgG (control). Bar = 100 mm. (b) Macroscopic view of the TEC, which was integrated to one spherical body. The diameter of this TEC was 5 mm and the thickness was 2 mm. (c) Microscopic view of HE staining (left side) and fibronectin staining (right side) of the cultured porcine chondral fragment for 7 days after the implantation of the basic TEC on the injured surface. Bar = 100 mm.
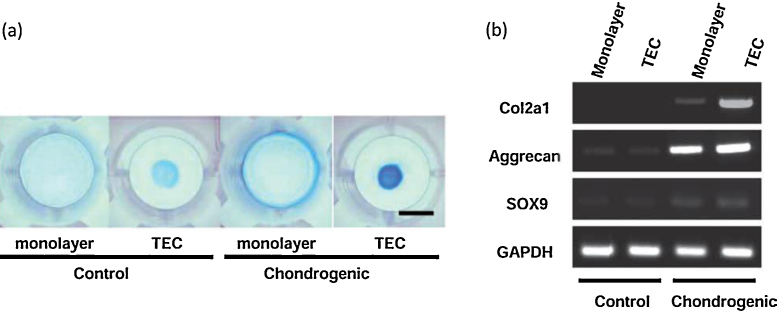
Chondrogenic differentiation potential of the TEC. (a) Alcian blue staining of monolayer cultured MSCs or a basic TEC in control medium or in the chondrogenic medium containing 500 ng/mL BMP2 for 14 days. Bar = 1 cm. (b) RT-PCR analysis of monolayer cultures or TEC for chondrogenic marker genes, type II collagen (COL2A1), aggrecan (ACAN), SOX9, and GAPDH.
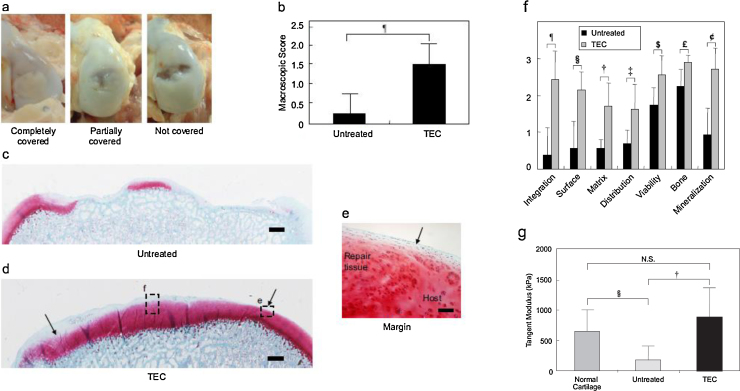
Macroscopical and histological assessment of in vivo TEC implantation on chondral defect. (a) Macroscopic view of porcine chondral lesion treated with or without the TEC at 6 months after implantation. When treated with the TEC, 4 of 8 defects are completely covered with repair tissue (left side) and the others are partially covered (middle). Without the TEC, most of the chondral lesions have little tissue coverage (right side). (b) Macroscopic score of the chondral lesion treated with (TEC, N = 8) or without (untreated, N = 4) TEC at 6 months. ¶: p = 0.017. (c, d) Safranin O staining of chondral lesion treated with (c) or without (d) the TEC at 6 months after operation. Bar = 1 mm. (e) Light magnification view in the area enclosed by dotted rectangle in (d) at the margin area. Bar = 100 mm. Note that the defect treated with the TEC is completely filled with repair tissue with good tissue integration to the adjacent cartilage and with restoration of smooth surface (arrow). In contrast, the chondral defect in the control group (c) shows osteoarthritic change with loss of cartilage and destruction of subchondral bone. Modified ICRS Visual Histological Assessment Scale of repair tissue treated with (TEC; N = 8) and without (untreated; N = 4) TEC. ¶: p = 0.009, §: p = 0.008, †: p = 0.010, ‡: p = 0.026, $: p = 0.037, £: p = 0.011, ¢: p = 0.006.
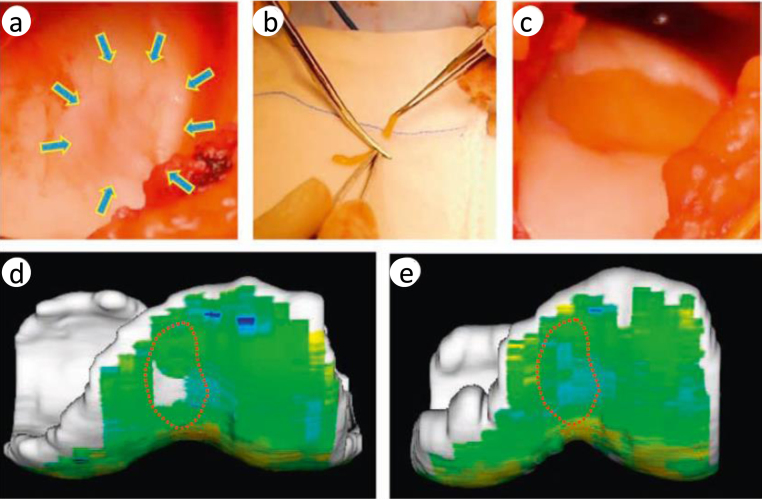
Arthroscopic and magnetic resonance imaging (MRI) analyses of repair tissue following implantation of a tissue-engineered construct (TEC) to repair human chondral defects in clinical trial. (a) A ICRS grade III lesion in the medial femoral chondyle after debridement. (b) Adjustment of the size of the TEC to match the lesion size just before implantation. (c) Implanted TEC into the lesion. (d, e) T2 mapping of the lesion at the femoral groove. (d) Before implantation and (e) 6 months after implantation.
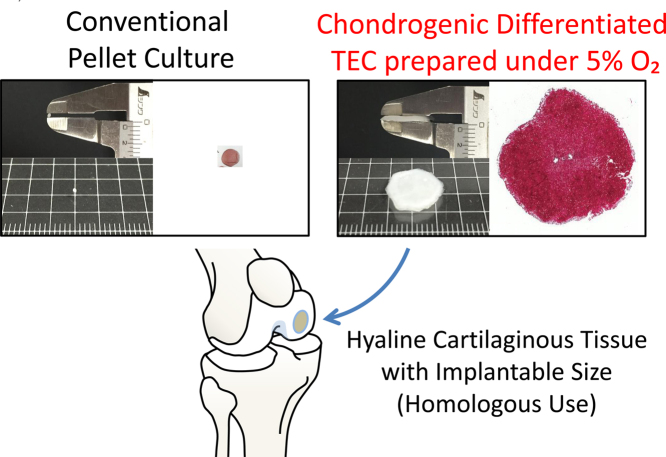
Schematic representation of homologous use of stem cell therapy using chondrogenic-differentiated TEC under low oxygen tension.
References
-
- Steadman J.R., Rodkey W.G., Rodrigo J.J. Microfracture: surgical technique and rehabilitation to treat chondral defects. Clin Orthop Relat Res. 2001:S362. - PubMed
-
- Gomoll A.H., Farr J., Gillogly S.D., Kercher J., Minas T. Surgical management of articular cartilage defects of the knee. J Bone Joint Surg Am. 2010;92:2470. - PubMed
-
- Moran C.J., Barry F.P., Maher S.A., Shannon F.J., Rodeo S.A. Advancing regenerative surgery in orthopaedic sports medicine: the critical role of the surgeon. Am J Sports Med. 2012;40:934. - PubMed
-
- Bae D.K., Yoon K.H., Song S.J. Cartilage healing after microfracture in osteoarthritic knees. Arthroscopy. 2006;22:367. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
