

Management of Supplemental Oxygen for Infants with Persistent Pulmonary Hypertension of Newborn: A Survey
- PMID: 27490772
- PMCID: PMC5646216
- DOI: 10.1055/s-0036-1586754
Management of Supplemental Oxygen for Infants with Persistent Pulmonary Hypertension of Newborn: A Survey
Abstract
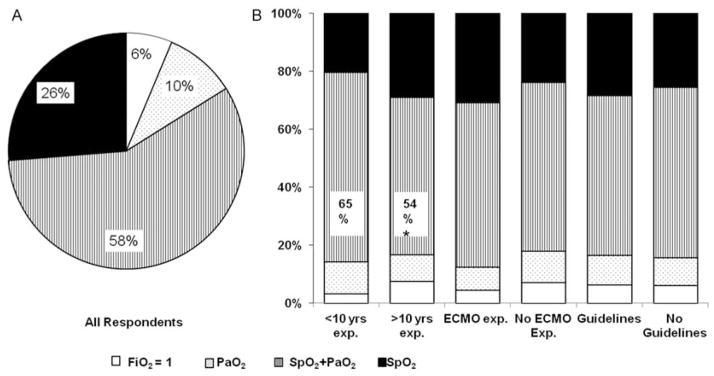
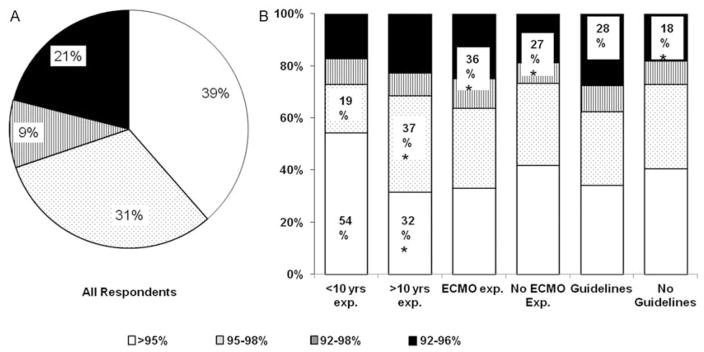
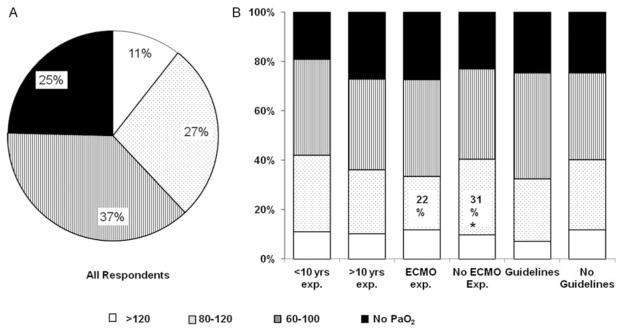
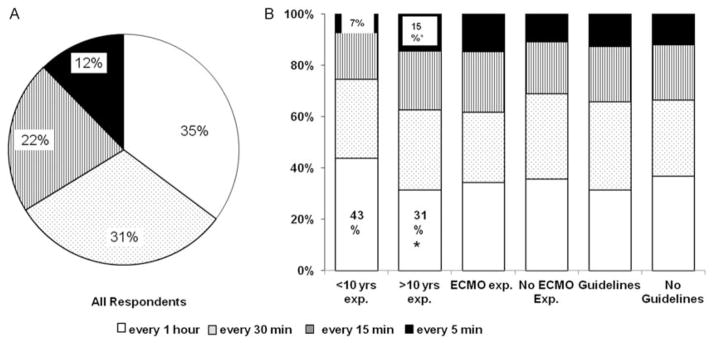
Objective To evaluate practice variations amongst neonatologists regarding oxygen management in neonates with persistent pulmonary hypertension of newborn (PPHN). Study Design An online survey was administered to neonatologists to assess goal oxygenation targets and oxygen titration practices in PPHN. Response variations were assessed and intergroup comparisons performed. Results Thirty-three percent (492) of neonatologists completed the survey. Twenty-eight percent reported using specific oxygen titration guidelines. Majority of respondents used a combination of oxygen saturation (SpO2) and arterial oxygen tension (PaO2) initially to titrate oxygen. Seventy percent of the respondents used higher goal SpO2 > 95% or 95 to 98% and thirty-eight percent of the respondents used PaO2 > 80 mm Hg. Physicians with extracorporeal membrane oxygenation experience and those with greater than ten years neonatal intensive care unit experience inclined toward use of SpO2 alone for oxygen titration and aimed for lower range of SpO2 and PaO2 targets. Greater proportion of neonatologists who employed specific oxygen titration guidelines used lower SpO2 targets. Conclusion Wide practice variations exist amongst neonatologists regarding optimal SpO2 and PaO2 targets and oxygen titration practices in the management of PPHN.
Thieme Medical Publishers 333 Seventh Avenue, New York, NY 10001, USA.
Figures
References
-
- Angus DC, Linde-Zwirble WT, Clermont G, Griffin MF, Clark RH. Epidemiology of neonatal respiratory failure in the United States: projections from California and New York. Am J Respir Crit Care Med. 2001;164(7):1154–1160. - PubMed
-
- Lipkin PH, Davidson D, Spivak L, Straube R, Rhines J, Chang CT. Neurodevelopmental and medical outcomes of persistent pulmonary hypertension in term newborns treated with nitric oxide. J Pediatr. 2002;140(3):306–310. - PubMed
-
- Walsh-Sukys MC, Tyson JE, Wright LL, et al. Persistent pulmonary hypertension of the newborn in the era before nitric oxide: practice variation and outcomes. Pediatrics. 2000;105(1 Pt 1):14–20. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
