

Diabetes and Cognitive Impairment
- PMID: 27491830
- PMCID: PMC5528145
- DOI: 10.1007/s11892-016-0775-x
Diabetes and Cognitive Impairment
Abstract
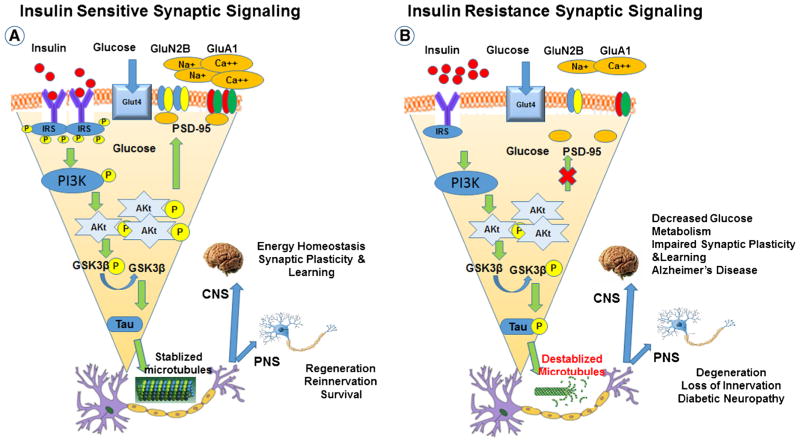
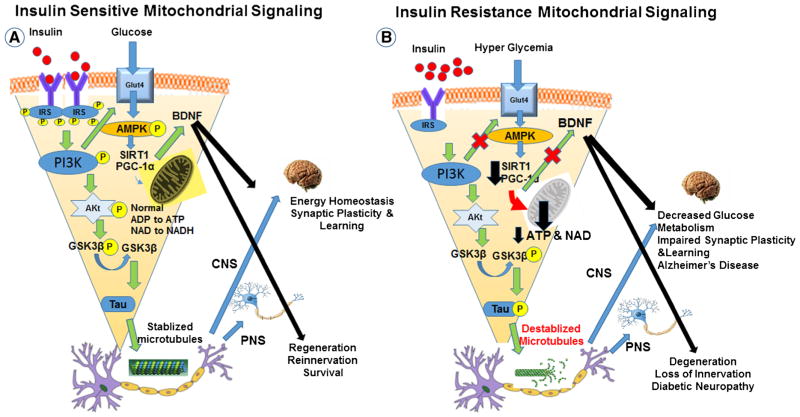
Both type 1 (T1DM) and type 2 diabetes mellitus (T2DM) have been associated with reduced performance on multiple domains of cognitive function and with evidence of abnormal structural and functional brain magnetic resonance imaging (MRI). Cognitive deficits may occur at the very earliest stages of diabetes and are further exacerbated by the metabolic syndrome. The duration of diabetes and glycemic control may have an impact on the type and severity of cognitive impairment, but as yet we cannot predict who is at greatest risk of developing cognitive impairment. The pathophysiology of cognitive impairment is multifactorial, although dysfunction in each interconnecting pathway ultimately leads to discordance in metabolic signaling. The pathophysiology includes defects in insulin signaling, autonomic function, neuroinflammatory pathways, mitochondrial (Mt) metabolism, the sirtuin-peroxisome proliferator-activated receptor-gamma co-activator 1α (SIRT-PGC-1α) axis, and Tau signaling. Several promising therapies have been identified in pre-clinical studies, but remain to be validated in clinical trials.
Keywords: Brain; Dementia; Diabetes; Encephalopathy; MRI; Mitochondria; Neuropathy; Treatment.
Figures
References
-
- Wong RH, Scholey A, Howe PR. Assessing premorbid cognitive ability in adults with type 2 diabetes mellitus—a review with implications for future intervention studies. Curr Diab Rep. 2014;14(11):547–0547. - PubMed
-
- Biessels GJ, Staekenborg S, Brunner E, Brayne C, Scheltens P. Risk of dementia in diabetes mellitus: a systematic review. Lancet Neurol. 2006;5(1):64–74. - PubMed
-
- Grunblatt E, Bartl J, Riederer P. The link between iron, metabolic syndrome, and Alzheimer’s disease. J Neural Transm. 2010;118(3):371–79. - PubMed
-
- Monette MC, Baird A, Jackson DL. A meta-analysis of cognitive functioning in nondemented adults with type 2 diabetes mellitus. Can J Diabetes. 2014;38(6):401–8. This study examines the pattern and magnitude of cognitive functioning deficits in persons withT2DM without dementia using meta-analysis. - PubMed
-
- Palta P, Schneider AL, Biessels GJ, Touradji P, Hill-Briggs F. Magnitude of cognitive dysfunction in adults with type 2 diabetes: a meta-analysis of six cognitive domains and the most frequently reported neuropsychological tests within domains. J Int Neuropsychol Soc. 2014;20(3):278–91. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
