

Modulation of endogenous antioxidant defense and the progression of kidney disease in multi-heritage groups of patients with type 2 diabetes: PRospective EValuation of Early Nephropathy and its Treatment (PREVENT)
- PMID: 27492324
- PMCID: PMC4973532
- DOI: 10.1186/s12967-016-0975-9
Modulation of endogenous antioxidant defense and the progression of kidney disease in multi-heritage groups of patients with type 2 diabetes: PRospective EValuation of Early Nephropathy and its Treatment (PREVENT)
Abstract
Background: Diabetes is the western world's leading cause of end-stage renal disease. Glucose-dependent, oxidative stress is linked to the development of renal inflammation and sclerosis, which, in animal models of diabetes, can be prevented by anti-oxidative treatment. Patients of non-Caucasian heritage have low activity of the selenoprotein, antioxidant enzyme, glutathione peroxidase (GPx) and its co-factor vitamin E, which may be linked to their increased propensity to developing end-stage renal disease.
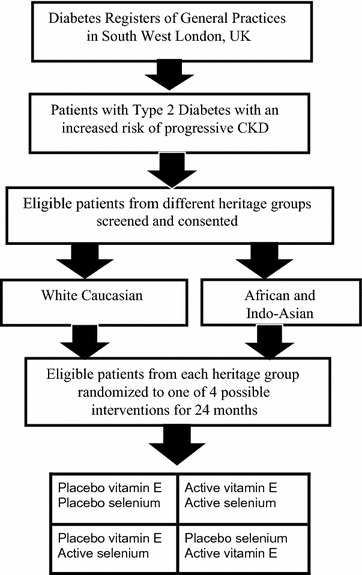
Research design and methods: We have designed a double-blind, randomized, placebo controlled study with selenium and/or vitamin E versus placebo as the interventions for patients with type 2 diabetes and chronic kidney disease (CKD) stages 1-3. A 2 × 2 factorial design will allow a balanced representation of the heritage groups exposed to each intervention. The primary biochemical outcome is change in GPx activity, and clinical outcome measure is the actual, rate of-and/or percentage change in estimated glomerular filtration rate (eGFR) from baseline. Analysis will be with a marginal model for longitudinal data using Generalized Estimating Equations corrected for measures of baseline serum antioxidant enzyme activities (GPx, superoxide dismutase and catalase), micronutrient levels (vitamins E and C), measures of inflammation (interleukin 6, c-reactive protein and monocyte chemoattractant protein-1) and markers of oxidative damage (plasma 8-isoprostaglandin F2α and urinary 8-hydroxydeoxyguanosine).
Expected results: The study will assess the relationship between GPx activity, oxidative stress, inflammation and eGFR. It will test the null hypothesis that antioxidant therapy does not influence the activity of GPx or other antioxidant enzymes and/or alter the rate of change in eGFR in these patient groups.
Conclusions: Outcome data on the effect of antioxidants in human diabetic renal disease is limited. Previous post hoc analyses have not shown a beneficial effect of vitamin E on renal function. A recent trial of a pharmaceutical antioxidant agent, improved eGFR, but in patients with advanced diabetes-related chronic kidney disease its use was associated with an increased incidence of cardiovascular events. We will explore whether the nutritional antioxidants, vitamin E and selenium alone, or in combination in patients at high risk of renal disease progression, forestalls a reduction in eGFR. The study will describe whether endogenous antioxidant enzyme defenses can be safely modified by this intervention and how this is associated with changes in markers of oxidative stress. Trial registration ISRCTN 97358113. Registered 21st September 2009.
Figures
References
-
- Babayev R, WhalyConnell A, Kshirsagar A, Klemmer P, Navaneethan S, Chen SC, Li S, McCulloough PA, Bakris G, Bomback A. KEEP Investigators. Association of race and body mass index with ESRD and mortality in CKD stages 3–4; results from the Kidney Early Evaluation Program (KEEP) Am J Kidney Dis. 2013;61(3):404–412. doi: 10.1053/j.ajkd.2012.11.038. - DOI - PubMed
-
- Chang TI, Li S, Chen SC, Peralta CA, Shlipak MG, Fried LF, et al. Risk factors for ESRD in individuals with preserved estimated GFR with and without albuminuria: results from the Kidney Early Evaluation Program (KEEP) Am J Kidney Dis. 2013;61(4 Suppl 2):S4–S11. doi: 10.1053/j.ajkd.2012.12.016. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
