

Common Functional Gastroenterological Disorders Associated With Abdominal Pain
- PMID: 27492916
- PMCID: PMC4985027
- DOI: 10.1016/j.mayocp.2016.06.003
Common Functional Gastroenterological Disorders Associated With Abdominal Pain
Abstract
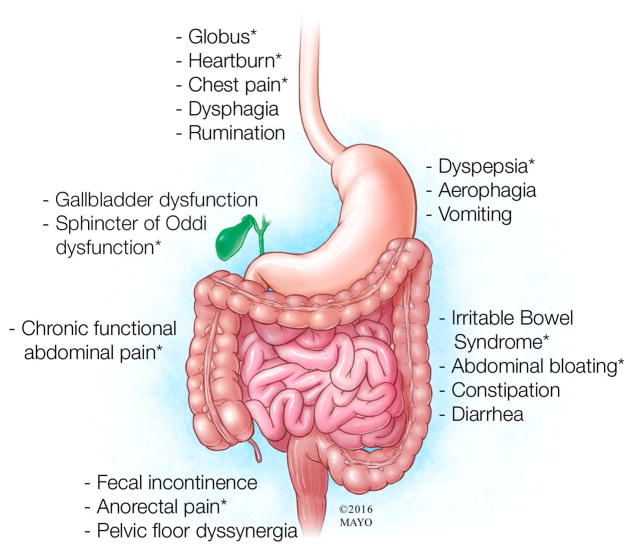
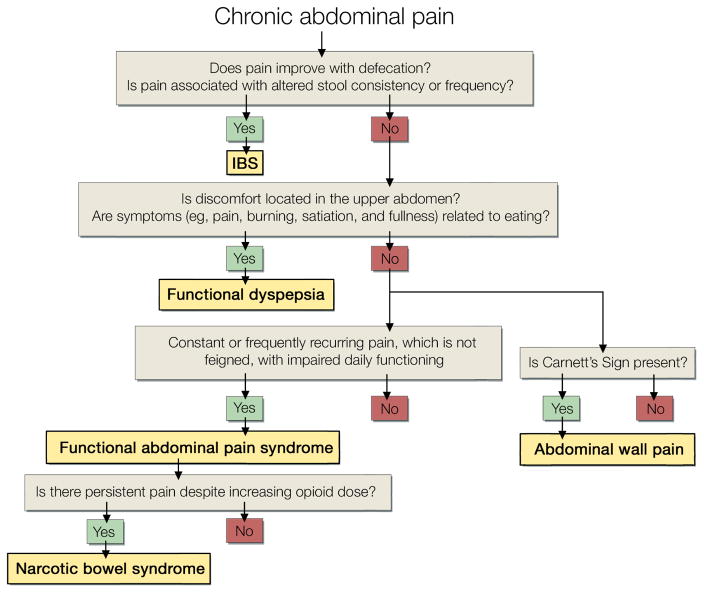
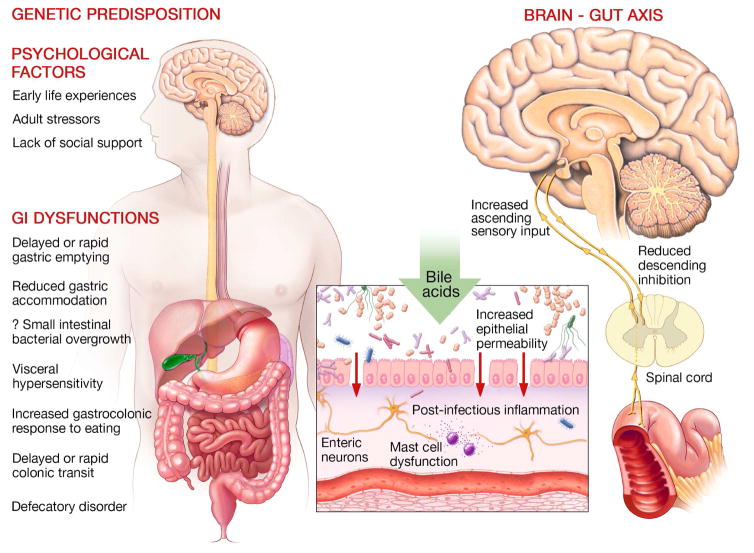
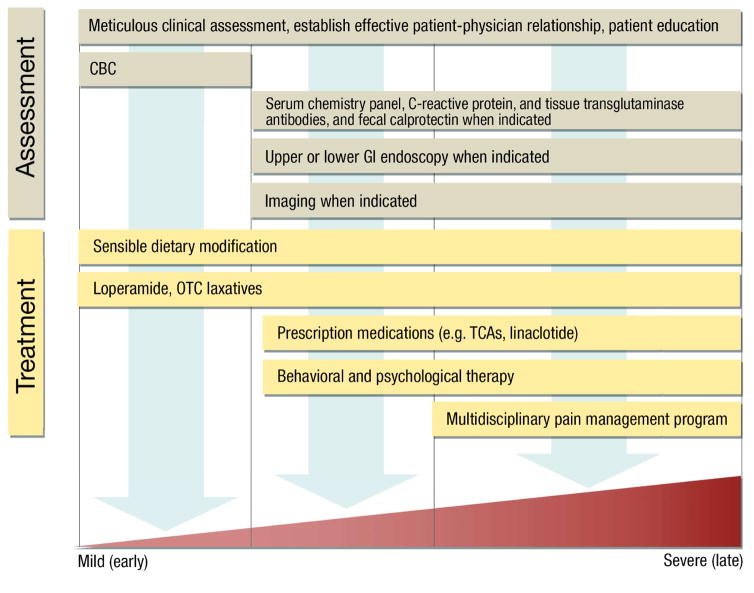
Although abdominal pain is a symptom of several structural gastrointestinal disorders (eg, peptic ulcer disease), this comprehensive review will focus on the 4 most common nonstructural, or functional, disorders associated with abdominal pain: functional dyspepsia, constipation-predominant and diarrhea-predominant irritable bowel syndrome, and functional abdominal pain syndrome. Together, these conditions affect approximately 1 in 4 people in the United States. They are associated with comorbid conditions (eg, fibromyalgia and depression), impaired quality of life, and increased health care utilization. Symptoms are explained by disordered gastrointestinal motility and sensation, which are implicated in various peripheral (eg, postinfectious inflammation and luminal irritants) and/or central (eg, stress and anxiety) factors. These disorders are defined and can generally be diagnosed by symptoms alone. Often prompted by alarm features, selected testing is useful to exclude structural disease. Identifying the specific diagnosis (eg, differentiating between functional abdominal pain and irritable bowel syndrome) and establishing an effective patient-physician relationship are the cornerstones of therapy. Many patients with mild symptoms can be effectively managed with limited tests, sensible dietary modifications, and over-the-counter medications tailored to symptoms. If these measures are not sufficient, pharmacotherapy should be considered for bowel symptoms (constipation or diarrhea) and/or abdominal pain; opioids should not be used. Behavioral and psychological approaches (eg, cognitive behavioral therapy) can be helpful, particularly in patients with chronic abdominal pain who require a multidisciplinary pain management program without opioids.
Copyright © 2016 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest: Dr. Bharucha reports personal fees from Allergan Inc, personal fees from Johnson and Johnson Inc, personal fees and other from Medspira, personal fees from Ironwood Pharma, personal fees from GI Care Pharma, personal fees from National Center for Pelvic Pain Research, personal fees from Salix, personal fees from Macmillan Medical Communications, personal fees from Forum Pharmaceuticals, outside the submitted work; In addition, Dr. Bharucha has a patent Anorectal manometry device with royalties paid to Medspira Inc, and a pending patent Anorectal manometry probe fixation device licensed to Medtronic Inc. Drs. Chakraborty and Sletten have nothing to disclose.
Figures
Comment in
-
Misdiagnosis of Diverticulitis in Patients With Irritable Bowel Syndrome.Mayo Clin Proc. 2016 Nov;91(11):1670-1671. doi: 10.1016/j.mayocp.2016.09.001. Mayo Clin Proc. 2016. PMID: 27814842 No abstract available.
References
-
- Drossman DA. The functional gastrointestinal disorders and the Rome III process. Gastroenterology. 2006;130(5):1377–1390. - PubMed
-
- Saito YA, Schoenfeld P, Locke GR., 3rd The epidemiology of irritable bowel syndrome in North America: a systematic review. Am J Gastroenterol. 2002;97(8):1910–1915. - PubMed
-
- Talley NJ, Ford AC. Functional Dyspepsia. N Engl J Med. 2015;373(19):1853–1863. - PubMed
-
- Clouse RE, Mayer EA, Aziz Q, et al. Functional abdominal pain syndrome. Gastroenterology. 2006;130(5):1492–1497. - PubMed
-
- Locke GR, 3rd, Yawn BP, Wollan PC, Melton LJ, 3rd, Lydick E, Talley NJ. Incidence of a clinical diagnosis of the irritable bowel syndrome in a United States population. Aliment Pharmacol Ther. 2004;19(9):1025–1031. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
