

Sarcopenic obesity and myosteatosis are associated with higher mortality in patients with cirrhosis
- PMID: 27493866
- PMCID: PMC4864157
- DOI: 10.1002/jcsm.12039
Sarcopenic obesity and myosteatosis are associated with higher mortality in patients with cirrhosis
Abstract
Background and aims: Obesity is frequently associated with cirrhosis, and cirrhotic patients may develop simultaneous loss of skeletal muscle and gain of adipose tissue, culminating in the condition of sarcopenic obesity. Additionally, muscle depletion is characterized by both a reduction in muscle size and increased proportion of muscular fat, termed myosteatosis. In this study, we aimed to establish the frequency and clinical significance of sarcopenia, sarcopenic obesity and myosteatosis in cirrhotic patients.
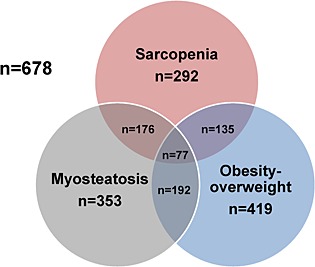
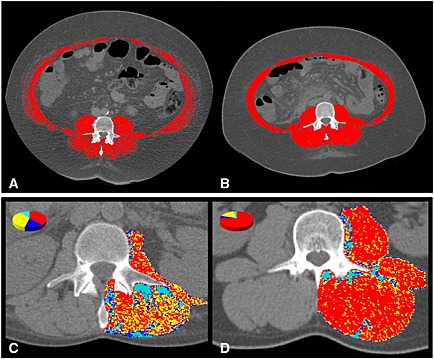
Methods: We analysed 678 patients with cirrhosis. Sarcopenia, sarcopenic obesity and myosteatosis were analysed by CT scan using the third lumbar vertebrae skeletal muscle and attenuation indexes, using previously validated gender-and body mass index-specific cutoffs.
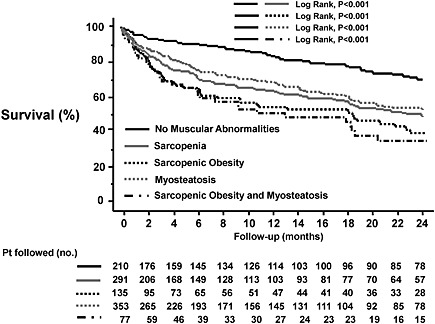
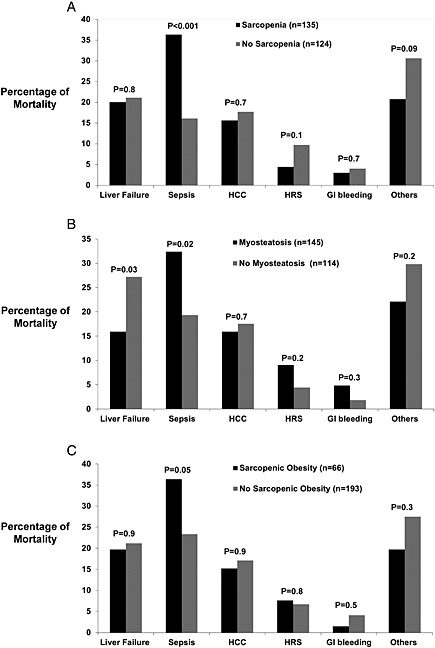
Results: Patients were predominately men (n = 457, 67%), and cirrhosis aetiology was hepatitis C virus in 269 patients (40%), alcohol in 153 (23%), non-alcoholic steatohepatitis/cryptogenic in 96 (14%), autoimmune liver disease in 55 (8%), hepatitis B virus in 43 (6%), and others in 5 patients (1%). Sarcopenia was present in 292 (43%), 135 had sarcopenic obesity (20%) and 353 had myosteatosis (52%). Patients with sarcopenia (22 ± 3 vs. 95 ± 22 months, P < 0.001), sarcopenic obesity (22 ± 3 vs. 95 ± 22 months, P < 0.001), and myosteatosis (28 ± 5 vs. 95 ± 22 months, P < 0.001) had worse median survival than patients without muscular abnormalities. By multivariate Cox regression analysis, both sarcopenia [hazard ratio (HR) 2.00, 95% confidence interval (CI) 1.44-2.77, P < 0.001], and myosteatosis (HR 1.42, 95% CI 1.02-1.07, P = 0.04) were associated with mortality.
Conclusions: Sarcopenia, sarcopenic obesity and myosteatosis are often present in patients with cirrhosis, and sarcopenia and myosteatosis are independently associated with a higher long-term mortality in cirrhosis.
Keywords: Cirrhosis; Lumbar skeletal muscle index; Muscle attenuation index; Muscle depletion; Myosteatosis; Overweight.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
