

Survival Benefit of Locoregional Treatment for Hepatocellular Carcinoma with Advanced Liver Cirrhosis
- PMID: 27493893
- PMCID: PMC4960362
- DOI: 10.1159/000367765
Survival Benefit of Locoregional Treatment for Hepatocellular Carcinoma with Advanced Liver Cirrhosis
Abstract
Background & aims: Hepatocellular carcinoma (HCC) with decompensated liver cirrhosis (LC) is a life-threatening condition, which is amenable to liver transplantation (LT) as the standard first-line treatment. However, the application of LT can be limited due to a shortage of donor livers. This study aimed to clarify the effect of non-surgical therapy on the survival of patients with HCC and decompensated LC.
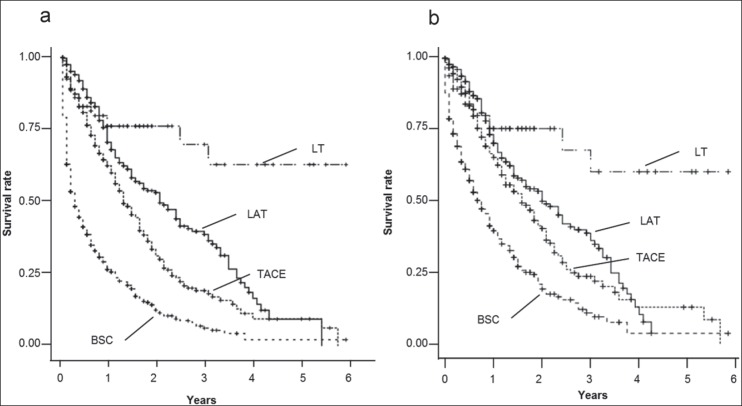
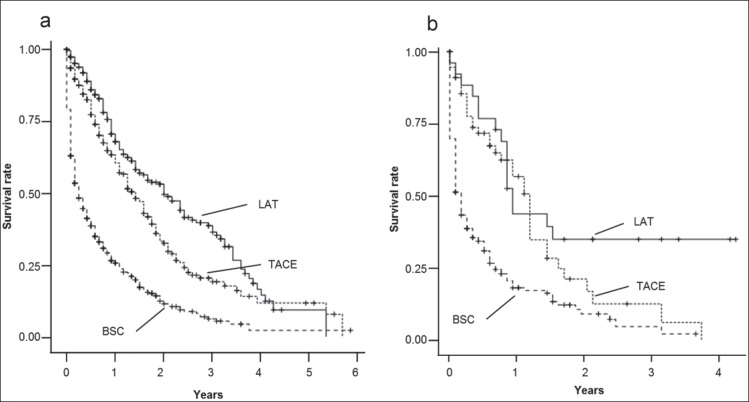
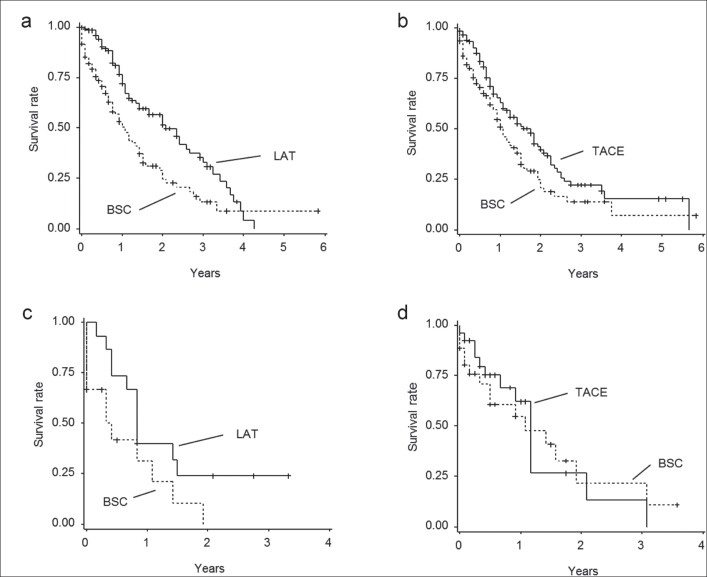
Methods: Of the 58,886 patients with HCC registered in the nationwide survey of the Liver Cancer Study Group of Japan (January 2000-December 2005), we included 1,344 patients with primary HCC and Child-Pugh (C-P) grade C for analysis in this retrospective study. Among the patients analyzed, 108 underwent LT, 273 were treated by local ablation therapy (LAT), 370 were treated by transarterial chemoembolization (TACE), and 593 received best supportive care (BSC). The effect of LT, LAT, and TACE on overall survival (OS) was analyzed using multivariate and propensity score analyses.
Results: Patient characteristics did not differ significantly between each treatment group and the BSC group, after propensity score matching. LAT (hazard ratio [HR]) =0.568; 95% confidence interval [CI], 0.40-0.80) and TACE (HR=0.691; 95% CI, 0.50-0.96) were identified as significant contributors to OS if the C-P score was less than 11 and tumor conditions met the Milan criteria.
Conclusions: For patients with HCC within the Milan criteria and with a C-P score of 10 or 11, locoregional treatment can be used as a salvage treatment if LT is not feasible.
Keywords: Best supportive care; Child-Pugh grade C; Local ablation therapy; Transarterial chemoembolization.
Figures
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Perz JF, Armstrong GL, Farrington LA, Hutin YJ, Bell BP. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol. 2006;45:529–538. - PubMed
-
- Infante-Rivard C, Esnaola S, Villeneuve JP. Clinical and statistical validity of conventional prognostic factors in predicting short-term survival among cirrhotics. Hepatology. 1987;7:660–664. - PubMed
-
- Kudo M, Chung H, Haji S, Osaki Y, Oka H, Seki T, Kasugai H, Sasaki Y, Matsunaga T. Validation of a new prognostic staging system for hepatocellular carcinoma: the JIS score compared with the CLIP score. Hepatology. 2004;40:1396–1405. - PubMed
-
- Kudo M, Izumi N, Kokudo N, Matsui O, Sakamoto M, Nakashima O, Kojiro M, Makuuchi M, HCC Expert Panel of Japan Society of Hepatology Management of hepatocellular carcinoma in Japan: Consensus-Based Clinical Practice Guidelines proposed by the Japan Society of Hepatology (JSH) 2010 updated version. Dig Dis. 2011;29:339–364. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
