

Respiratory Muscle Strength as a Predictive Biomarker for Survival in Amyotrophic Lateral Sclerosis
- PMID: 27494149
- PMCID: PMC5214920
- DOI: 10.1164/rccm.201604-0848OC
Respiratory Muscle Strength as a Predictive Biomarker for Survival in Amyotrophic Lateral Sclerosis
Abstract
Rationale: Biomarkers for survival in amyotrophic lateral sclerosis (ALS) would facilitate the development of novel drugs. Although respiratory muscle weakness is a known predictor of poor prognosis, a comprehensive comparison of different tests is lacking.
Objectives: To compare the predictive power of invasive and noninvasive respiratory muscle strength assessments for survival or ventilator-free survival, up to 3 years.
Methods: From a previously published report respiratory muscle strength measurements were available for 78 patients with ALS. Time to death and/or ventilation were ascertained. Receiver operating characteristic analysis was used to determine the cutoff point of each parameter.
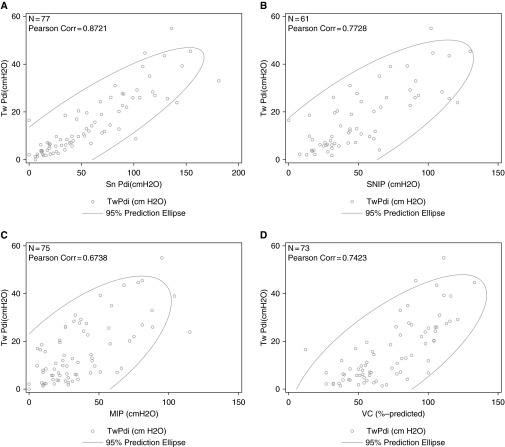
Measurements and main results: Each respiratory muscle strength assessment individually achieved statistical significance for prediction of survival or ventilator-free survival. In multivariate analysis sniff trans-diaphragmatic and esophageal pressure, twitch trans-diaphragmatic pressure (Tw Pdi), age, and maximal static expiratory mouth pressure were significant predictors of ventilation-free survival and Tw Pdi and maximal static expiratory mouth pressure for absolute survival. Although all measures had good specificity, there were differing sensitivities. All cutoff points for the VC were greater than 80% of normal, except for prediction of 3-month outcomes. Sequential data showed a linear decline for direct measures of respiratory muscle strength, whereas VC showed little to no decline until 12 months before death/ventilation.
Conclusions: The most powerful biomarker for mortality stratification was Tw Pdi, but the predictive power of sniff nasal inspiratory pressure was also excellent. A VC within normal range suggested a good prognosis at 3 months but was of little other value.
Keywords: amyotrophic lateral sclerosis; diaphragm; maximal inspiratory pressure; sniff nasal inspiratory pressure; survival.
Figures



Comment in
-
Respiratory Muscle Strength: A Reliable Index for Predicting Survival in Amyotrophic Lateral Sclerosis?Am J Respir Crit Care Med. 2017 Jan 1;195(1):12-13. doi: 10.1164/rccm.201608-1697ED. Am J Respir Crit Care Med. 2017. PMID: 28035847 No abstract available.
-
Predicting Survival in Amyotrophic Lateral Sclerosis: Should We Move Forward from Vital Capacity?Am J Respir Crit Care Med. 2017 Jan 1;195(1):144-145. doi: 10.1164/rccm.201609-1838LE. Am J Respir Crit Care Med. 2017. PMID: 28035853 No abstract available.
References
-
- Lacomblez L, Bensimon G, Leigh PN, Guillet P, Meininger V Amyotrophic Lateral Sclerosis/Riluzole Study Group II. Dose-ranging study of riluzole in amyotrophic lateral sclerosis. Lancet. 1996;347:1425–1431. - PubMed
-
- Bourke SC, Tomlinson M, Williams TL, Bullock RE, Shaw PJ, Gibson GJ. Effects of non-invasive ventilation on survival and quality of life in patients with amyotrophic lateral sclerosis: a randomised controlled trial. Lancet Neurol. 2006;5:140–147. - PubMed
-
- Lyall RA, Donaldson N, Fleming T, Wood C, Newsom-Davis I, Polkey MI, Leigh PN, Moxham J. A prospective study of quality of life in ALS patients treated with noninvasive ventilation. Neurology. 2001;57:153–156. - PubMed
-
- Lyall RA, Donaldson N, Polkey MI, Leigh PN, Moxham J. Respiratory muscle strength and ventilatory failure in amyotrophic lateral sclerosis. Brain. 2001;124:2000–2013. - PubMed
-
- Haverkamp LJ, Appel V, Appel SH. Natural history of amyotrophic lateral sclerosis in a database population. Validation of a scoring system and a model for survival prediction. Brain. 1995;118:707–719. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
