

Aponeurosis of the levator palpebrae superioris in Chinese subjects: A live gross anatomy and cadaveric histological study
- PMID: 27495084
- PMCID: PMC4979838
- DOI: 10.1097/MD.0000000000004469
Aponeurosis of the levator palpebrae superioris in Chinese subjects: A live gross anatomy and cadaveric histological study
Abstract
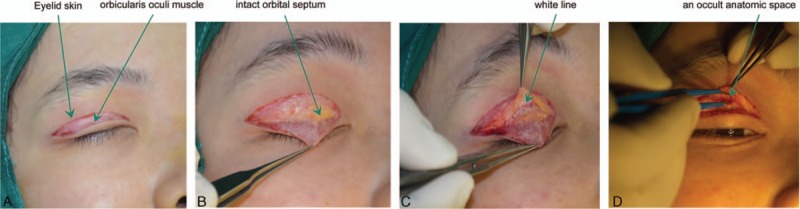
An accurate understanding of the anatomy of the levator palpebrae superioris aponeurosis (LPSA) is critical for successful blepharoplasty of aponeurotic ptosis. We investigated the macroscopic and microscopic anatomy of the LPSA.This prospective live gross anatomy study enrolled 200 adult Chinese patients with bilateral mild ptosis undergoing elective blepharoplasty. Full-thick eyelid tissues and sagittal sections from the eyelid skin to the conjunctiva were examined with Masson trichrome staining or antismooth muscle actin (SMA) immunohistochemistry.Gross anatomy showed that the space between the superficial and deep layers of the LPSA could be accessed after incising the overlying superficial fascia, by retracting the white line. Adipose layers were clearly observed in 195 out of 200 patients with bilateral mild ptosis, among which 180 cases had the superficial layer connected to the uncoated adipose. Fifteen cases had the superficial layer connected to the smoothly coated layer, and 5 cases had the superficial layer directly connected to the deep loose fiber, almost without adipose. In previously untreated patients, the LPSA space was located beneath the intact orbital septum. In those with previous surgeries, it was beneath the superficial layer of the LPSA, underlying the destructed orbital septum. Cadaveric histology showed that the deep layer of the LPSA extended into the anterior layer of the tarsal plate and the superficial layer reflexed upward in continuity with the vertical orbital septum. An occult space existed between the 2 layers of the LPSA, with a smooth lining on the deep layer. The superficial layer of the LPSA was SMA-immunonegative but the deep layer was slightly immunopositive for SMA. An occult anatomic space exists between the superficial and deep layers of the LPSA, in proximity to the superior tarsal plate margin. Recognition of the more anatomically significant LPSA deep layer may help improve the aesthetic outcome of blepharoplasty.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures




References
-
- Nam YS, Kim IB, Shin SY. Detailed anatomy of the transverse superior fascial expansion of the upper eyelid. Graefes Arch Clin Exp Ophthalmol 2015; 253:633–636. - PubMed
-
- Stasior GO, Lemke BN, Wallow IH, et al. Levator aponeurosis elastic fiber network. Ophthal Plast Reconstr Surg 1993; 9:1–10. - PubMed
-
- Meyer DR, Linberg JV, Wobig JL, et al. Anatomy of the orbital septum and associated eyelid connective tissues. Implications for ptosis surgery. Ophthal Plast Reconstr Surg 1991; 7:104–113. - PubMed
-
- Bremond-Gignac DS, Deplus S, Cussenot O, et al. Anatomic study of the orbital septum (22.10.93). Surg Radiol Anat 1994; 16:121–124. - PubMed
-
- Zide BM. Anatomy of the eyelids. Clin Plast Surg 1981; 8:623–634. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
