

Washed cell salvage in surgical patients: A review and meta-analysis of prospective randomized trials under PRISMA
- PMID: 27495095
- PMCID: PMC4979849
- DOI: 10.1097/MD.0000000000004490
Washed cell salvage in surgical patients: A review and meta-analysis of prospective randomized trials under PRISMA
Erratum in
-
Washed cell salvage in surgical patients: A review and meta-analysis of prospective randomized trials under PRISMA: Erratum.Medicine (Baltimore). 2018 Apr;97(17):e0640. doi: 10.1097/MD.0000000000010640. Medicine (Baltimore). 2018. PMID: 29703066 Free PMC article. No abstract available.
Abstract
Background: Cell salvage is commonly used as part of a blood conservation strategy. However concerns among clinicians exist about the efficacy of transfusion of washed cell salvage.
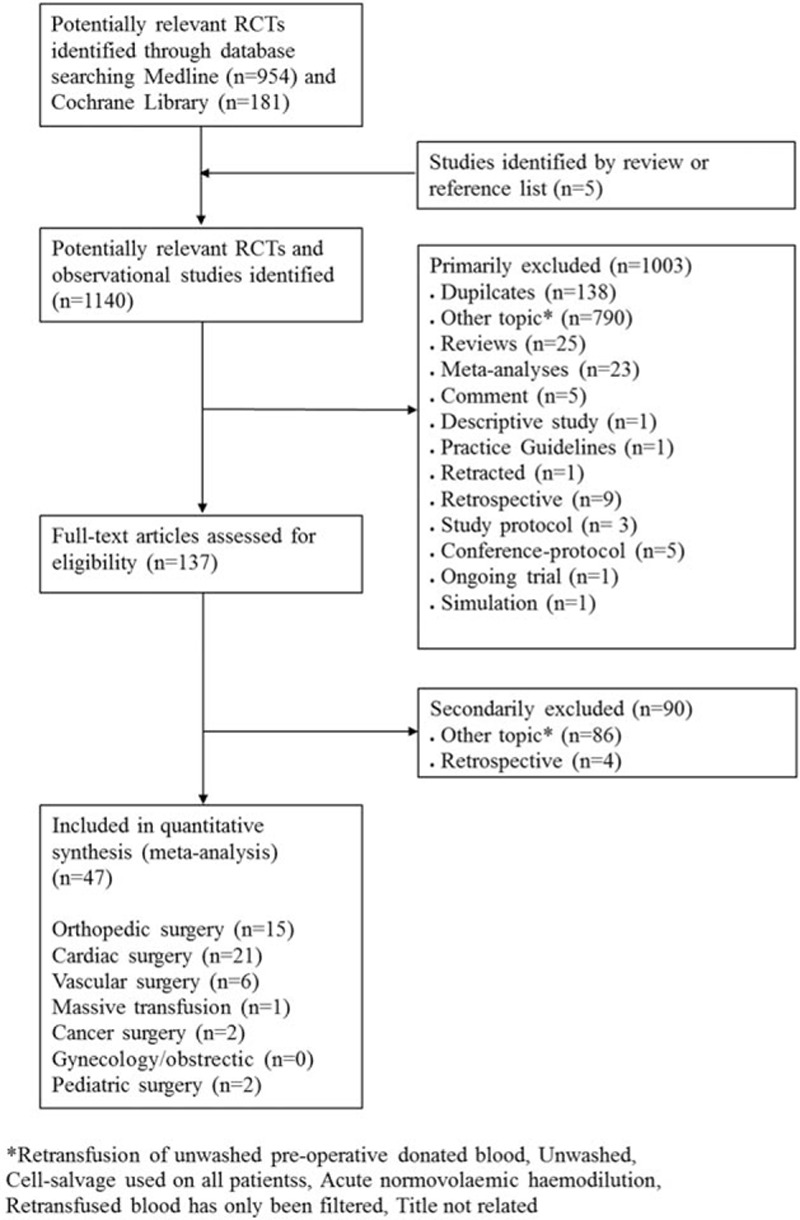
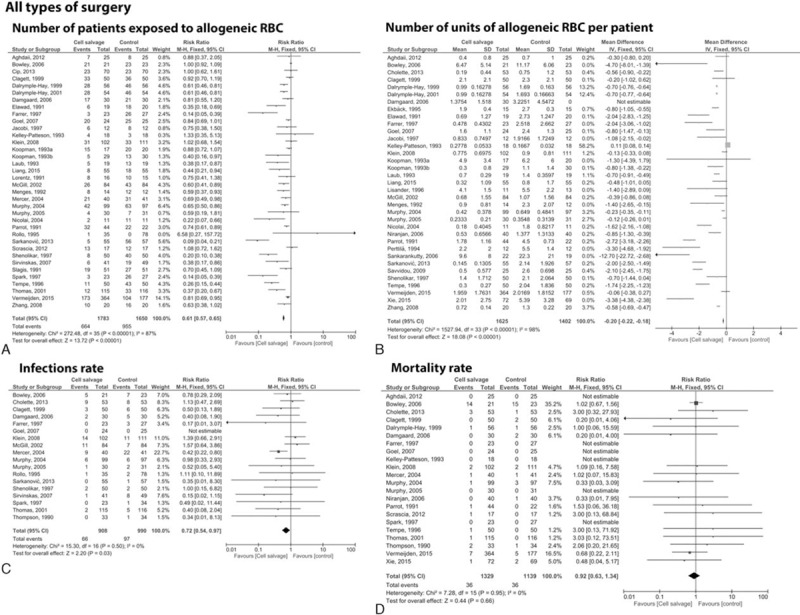
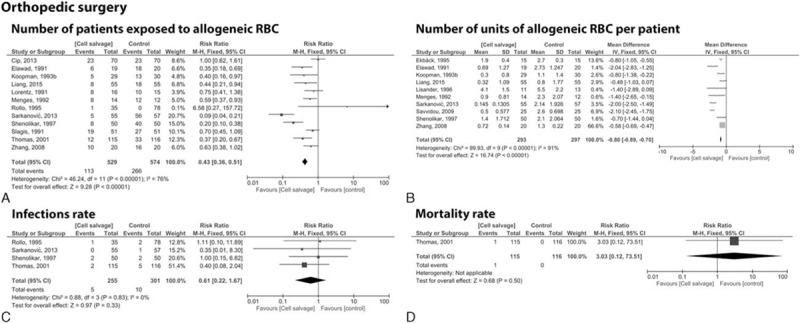
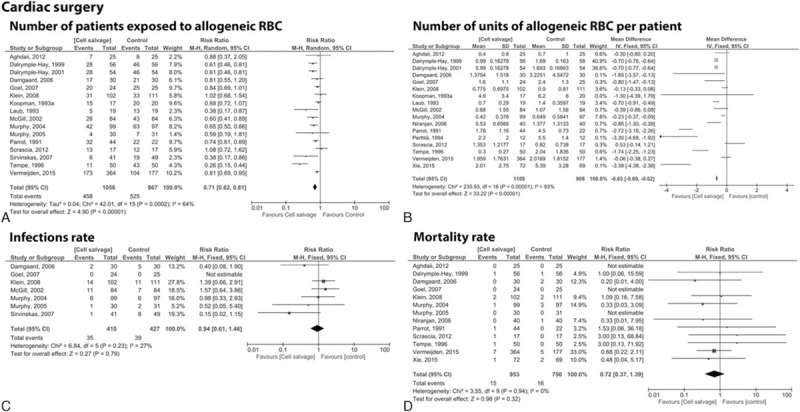
Methods: We performed a meta-analysis of randomized controlled trials in which patients, scheduled for all types of surgery, were randomized to washed cell salvage or to a control group with no cell salvage. Data were independently extracted, risk ratio (RR), and weighted mean differences (WMD) with 95% confidence intervals (CIs) were calculated. Data were pooled using a random effects model. The primary endpoint was the number of patients exposed to allogeneic red blood cell (RBC) transfusion.
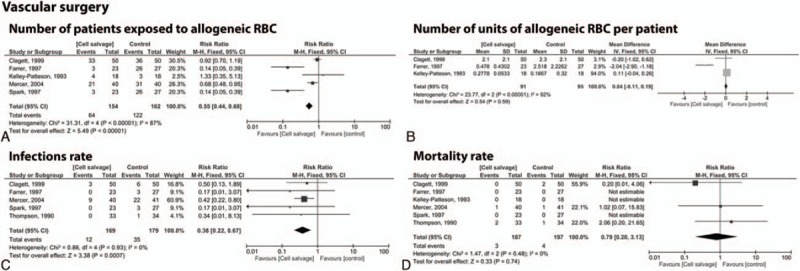
Results: Out of 1140 search results, a total of 47 trials were included. Overall, the use of washed cell salvage reduced the rate of exposure to allogeneic RBC transfusion by a relative 39% (RR = 0.61; 95% CI 0.57 to 0.65; P < 0.001), resulting in an average saving of 0.20 units of allogeneic RBC per patient (weighted mean differences [WMD] = -0.20; 95% CI -0.22 to -0.18; P < 0.001), reduced risk of infection by 28% (RR = 0.72; 95% CI 0.54 to 0.97; P = 0.03), reduced length of hospital stay by 2.31 days (WMD = -2.31; 95% CI -2.50 to -2.11; P < 0.001), but did not significantly affect risk of mortality (RR = 0.92; 95% CI 0.63 to 1.34; P = 0.66). No statistical difference could be observed in the number of patients exposed to re-operation, plasma, platelets, or rate of myocardial infarction and stroke.
Conclusions: Washed cell salvage is efficacious in reducing the need for allogeneic RBC transfusion and risk of infection in surgery.
Conflict of interest statement
Disclosure of Conflict: PM and KZ received honoraria from the following companies for conducting a large clinical cohort trial in the field of Patient Blood Management: Vifor Pharma Deutschland GmbH, Muenchen, Germany; B. Braun Melsungen AG, Melsungen, Germany; CSL Behring, Marburg, Germany; and Fresenius Kabi, Bad Homburg, Germany. DRS: Dr Spahn's academic department is/has been receiving grant support from the Swiss National Science Foundation, Berne, Switzerland, the Ministry of Health (Gesundheitsdirektion) of the Canton of Zurich, Switzerland for Highly Specialized Medicine, the Swiss Society of Anesthesiology and Reanimation (SGAR), Berne, Switzerland, the Swiss Foundation for Anesthesia Research, Zurich, Switzerland, Bundesprogramm Chancengleichheit, Berne, Switzerland, CSL Behring, Berne, Switzerland, Vifor SA, Villars-sur-Glâne, Switzerland. DRS was the chairman of the ABC Faculty and is the co-chairman of the ABC-Trauma Faculty, which both are managed by Physicians World Europe GmbH, Mannheim, Germany and sponsored by unrestricted educational grants from Novo Nordisk Health Care AG, Zurich, Switzerland, CSL Behring GmbH, Marburg, Germany and LFB Biomédicaments, Courtaboeuf Cedex, France. In the past 5 years, DRS has received honoraria or travel support for consulting or lecturing from the following companies: Abbott AG, Baar, Switzerland, AMGEN GmbH, Munich, Germany, AstraZeneca AG, Zug, Switzerland, Baxter AG, Volketswil, Switzerland, Baxter S.p.A., Roma, Italy, Bayer (Schweiz) AG, Zürich, Switzerland, Bayer Pharma AG, Berlin, Germany, B. Braun Melsungen AG, Melsungen, Germany, Boehringer Ingelheim (Schweiz) GmbH, Basel, Switzerland, Bristol-Myers-Squibb, Rueil-Malmaison Cedex, France and Baar, Switzerland, CSL Behring GmbH, Hattersheim am Main, Germany and Berne, Switzerland, Curacyte AG, Munich, Germany, Daiichi Sankyo (Schweiz) AG, Thalwil, Switzerland, Ethicon Biosurgery, Sommerville, New Jersey, USA, Fresenius SE, Bad Homburg v.d.H., Germany, Galenica AG, Bern, Switzerland (including Vifor SA, Villars-sur-Glâne, Switzerland), GlaxoSmithKline GmbH & Co. KG, Hamburg, Germany, Janssen-Cilag AG, Baar, Switzerland, Janssen-Cilag EMEA, Beerse, Belgium, LFB Biomédicaments, Courtaboeuf Cedex, France, Merck Sharp & Dohme AG, Luzern, Switzerland, Novo Nordisk A/S, Bagsvärd, Denmark, Octapharma AG, Lachen, Switzerland, Organon AG, Pfäffikon/SZ, Switzerland, Oxygen Biotherapeutics, Costa Mesa, CA, PAION Deutschland GmbH, Aachen, Germany, Pharmacosmos A/S, Holbaek, Denmark, Photonics Healthcare B.V., Utrecht, Netherlands, ratiopharm Arzneimittel Vertriebs-GmbH, Vienna, Austria, Roche Diagnostics International Ltd, Reinach, Switzerland, Roche Pharma (Schweiz) AG, Reinach, Switzerland, Schering-Plough International, Inc., Kenilworth, New Jersey, USA, Tem International GmbH, Munich, Germany, Verum Diagnostica GmbH, Munich, Germany, Vifor Pharma Deutschland GmbH, Munich, Germany, Vifor Pharma Österreich GmbH, Vienna, Austria, Vifor (International) AG, St. Gallen, Switzerland. The remaining author has no conflicts of interest.
Figures
References
-
- Glance LG, Dick AW, Mukamel DB, et al. Association between intraoperative blood transfusion and mortality and morbidity in patients undergoing noncardiac surgery. Anesthesiology 2011; 114:283–292. - PubMed
-
- Shander A, Fink A, Javidroozi M, et al. Appropriateness of allogeneic red blood cell transfusion: the international consensus conference on transfusion outcomes. Transfus Med Rev 2011; 25:232.e53–246.e53. - PubMed
-
- Carless PA, Henry DA, Moxey AJ, et al. Cell salvage for minimising perioperative allogeneic blood transfusion. Cochrane Database Syst Rev 2010; Cd001888. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
