

Probiotics for prevention and treatment of respiratory tract infections in children: A systematic review and meta-analysis of randomized controlled trials
- PMID: 27495104
- PMCID: PMC4979858
- DOI: 10.1097/MD.0000000000004509
Probiotics for prevention and treatment of respiratory tract infections in children: A systematic review and meta-analysis of randomized controlled trials
Abstract
Background: Respiratory tract infections (RTIs) represent one of the main health problems in children. Probiotics are viable bacteria that colonize the intestine and affect the host intestinal microbial balance. Accumulating evidence suggests that probiotic consumption may decrease the incidence of or modify RTIs. The authors systematically reviewed data from randomized controlled trials (RCTs) to investigate the effect of probiotic consumption on RTIs in children.
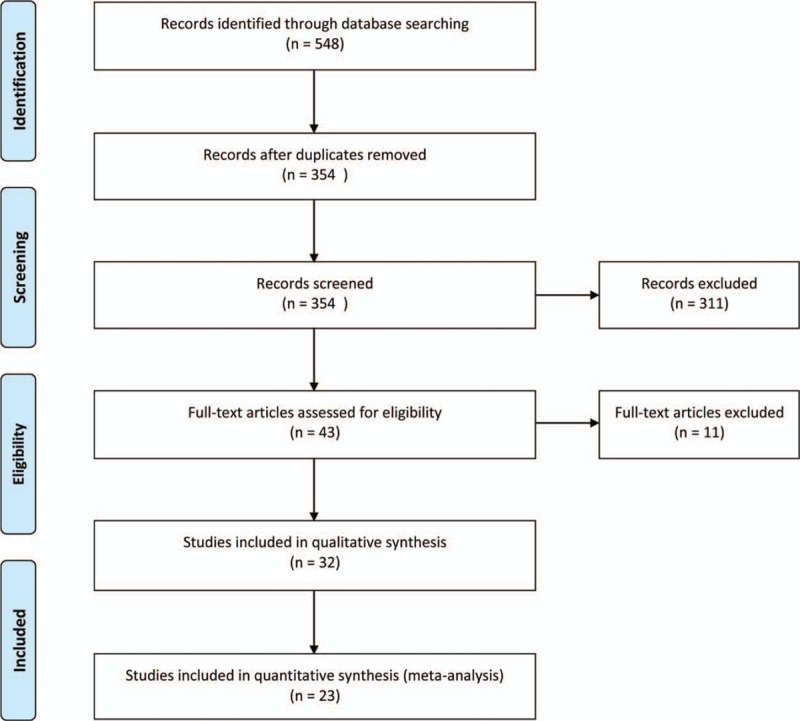
Methods: MEDLINE/PubMed, Embase, Cochrane Library, and Web of Science were systematically searched for RCTs regarding the effect of probiotics on RTIs in children. The outcomes included number of children experienced with at least 1 RTI episode, duration of illness episodes, days of illness per subject, and school/day care absenteeism due to infection. A random-effects model was used to calculate pooled relative risks, or mean difference (MD) with the corresponding 95% confidence interval (CI).
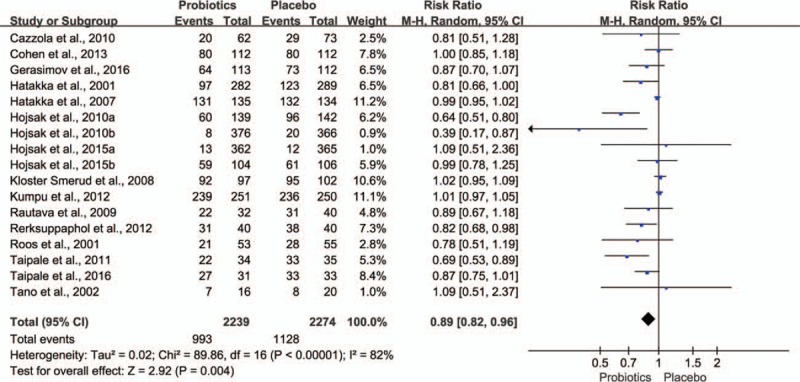
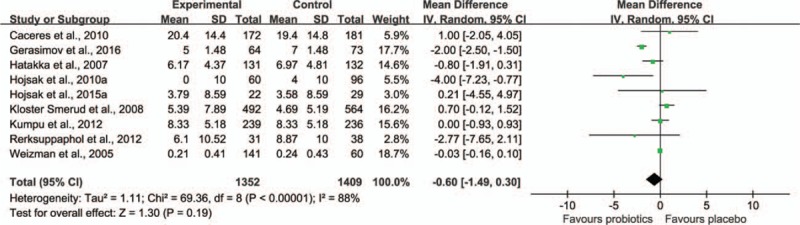
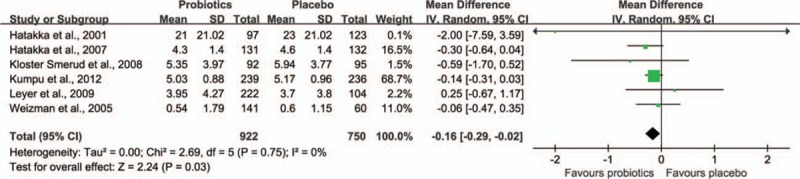
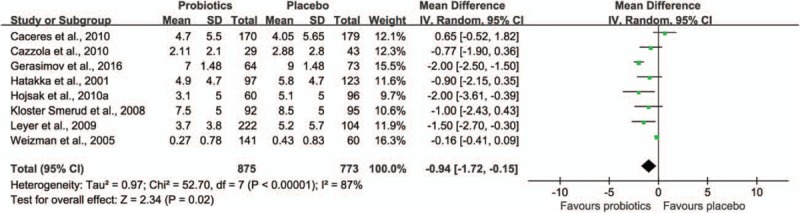
Results: A total of 23 trials involving 6269 children were eligible for inclusion in the systematic review. None of the trials showed a high risk of bias. The quality of the evidence of outcomes was moderate. The age range of subjects was from newborn to 18 years. The results of meta-analysis showed that probiotic consumption significantly decreased the number of subjects having at least 1 RTI episode (17 RCTs, 4513 children, relative risk 0.89, 95% CI 0.82-0.96, P = 0.004). Children supplemented with probiotics had fewer numbers of days of RTIs per person compared with children who had taken a placebo (6 RCTs, 2067 children, MD -0.16, 95% CI -0.29 to 0.02, P = 0.03), and had fewer numbers of days absent from day care/school (8 RCTs, 1499 children, MD -0.94, 95% CI -1.72 to -0.15, P = 0.02). However, there was no statistically significant difference of illness episode duration between probiotic intervention group and placebo group (9 RCTs, 2817 children, MD -0.60, 95% CI -1.49 to 0.30, P = 0.19).
Conclusion: Based on the available data and taking into account the safety profile of RCTs, probiotic consumption appears to be a feasible way to decrease the incidence of RTIs in children.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Vesa S, Kleemola M, Blomqvist S, et al. Epidemiology of documented viral respiratory infections and acute otitis media in a cohort of children followed from two to twenty-four months of age. Pediatr Infect Dis J 2001; 20:574–581. - PubMed
-
- Nokso-Koivisto J, Pitkaranta A, Blomqvist S, et al. Viral etiology of frequently recurring respiratory tract infections in children. Clin Infect Dis 2002; 35:540–546. - PubMed
-
- Nicholson KG, McNally T, Silverman M, et al. Rates of hospitalisation for influenza, respiratory syncytial virus and human metapneumovirus among infants and young children. Vaccine 2006; 24:102–108. - PubMed
-
- Massin MM, Montesanti J, Gerard P, et al. Spectrum and frequency of illness presenting to a pediatric emergency department. Acta Clin Belg 2006; 61:161–165. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
