

Behavioral interventions to reduce inappropriate antibiotic prescribing: a randomized pilot trial
- PMID: 27495917
- PMCID: PMC4975897
- DOI: 10.1186/s12879-016-1715-8
Behavioral interventions to reduce inappropriate antibiotic prescribing: a randomized pilot trial
Abstract
Background: Clinicians frequently prescribe antibiotics inappropriately for acute respiratory infections (ARIs). Our objective was to test information technology-enabled behavioral interventions to reduce inappropriate antibiotic prescribing for ARIs in a randomized controlled pilot test trial.
Methods: Primary care clinicians were randomized in a 2 × 2 × 2 factorial experiment with 3 interventions: 1) Accountable Justifications; 2) Suggested Alternatives; and 3) Peer Comparison. Beforehand, participants completed an educational module. Measures included: rates of antibiotic prescribing for: non-antibiotic-appropriate ARI diagnoses, acute sinusitis/pharyngitis, all other diagnoses/symptoms of respiratory infection, and all three ARI categories combined.
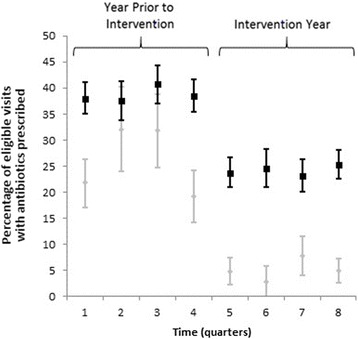
Results: We examined 3,276 visits in the pre-intervention year and 3,099 in the intervention year. The antibiotic prescribing rate fell for non-antibiotic-appropriate ARIs (24.7 % in the pre-intervention year to 5.2 % in the intervention year); sinusitis/pharyngitis (50.3 to 44.7 %); all other diagnoses/symptoms of respiratory infection (40.2 to 25.3 %); and all categories combined (38.7 to 24.2 %; all p < 0.001). There were no significant relationships between any intervention and antibiotic prescribing for non-antibiotic-appropriate ARI diagnoses or sinusitis/pharyngitis. Suggested Alternatives was associated with reduced antibiotic prescribing for other diagnoses or symptoms of respiratory infection (odds ratio [OR], 0.62; 95 % confidence interval [CI], 0.44-0.89) and for all ARI categories combined (OR, 0.72; 95 % CI, 0.54-0.96). Peer Comparison was associated with reduced prescribing for all ARI categories combined (OR, 0.73; 95 % CI, 0.53-0.995).
Conclusions: We observed large reductions in antibiotic prescribing regardless of whether or not study participants received an intervention, suggesting an overriding Hawthorne effect or possibly clinician-to-clinician contamination. Low baseline inappropriate prescribing may have led to floor effects.
Trial registration: ClinicalTrials.gov: NCT01454960 .
Keywords: Acute respiratory infections; Antibiotics; Behavioral economics; Clinical decision support; Social psychology.
Figures
References
-
- Centers for Disease Control and Prevention. Antibiotic Resistance Threats in the United States, 2013. http://www.cdc.gov/drugresistance/threat-report-2013/. Accessed 28 Jul 2015.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
