

mHealth Intervention to Improve Diabetes Risk Behaviors in India: A Prospective, Parallel Group Cohort Study
- PMID: 27496271
- PMCID: PMC4992169
- DOI: 10.2196/jmir.5712
mHealth Intervention to Improve Diabetes Risk Behaviors in India: A Prospective, Parallel Group Cohort Study
Abstract
Background: In low/middle income countries like India, diabetes is prevalent and health care access limited. Most adults have a mobile phone, creating potential for mHealth interventions to improve public health. To examine the feasibility and initial evidence of effectiveness of mDiabetes, a text messaging program to improve diabetes risk behaviors, a global nonprofit organization (Arogya World) implemented mDiabetes among one million Indian adults.
Objective: A prospective, parallel cohort design was applied to examine whether mDiabetes improved fruit, vegetable, and fat intakes and exercise.
Methods: Intervention participants were randomly selected from the one million Nokia subscribers who elected to opt in to mDiabetes. Control group participants were randomly selected from non-Nokia mobile phone subscribers. mDiabetes participants received 56 text messages in their choice of 12 languages over 6 months; control participants received no contact. Messages were designed to motivate improvement in diabetes risk behaviors and increase awareness about the causes and complications of diabetes. Participant health behaviors (exercise and fruit, vegetable, and fat intake) were assessed between 2012 and 2013 via telephone surveys by blinded assessors at baseline and 6 months later. Data were cleaned and analyzed in 2014 and 2015.
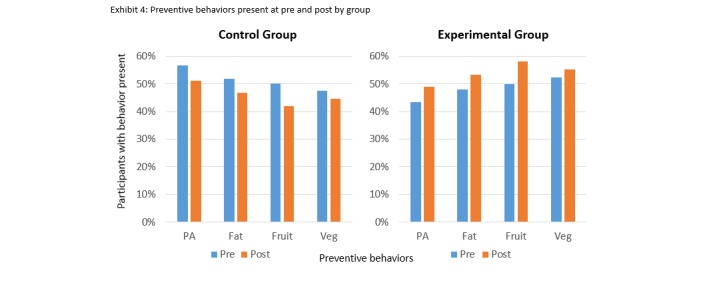
Results: 982 participants in the intervention group and 943 in the control group consented to take the phone survey at baselne. At the end of the 6-month period, 611 (62.22%) in the intervention and 632 (67.02%) in the control group completed the follow-up telephone survey. Participants receiving texts demonstrated greater improvement in a health behavior composite score over 6 months, compared with those who received no messages F(1, 1238) = 30.181, P<.001, 95% CI, 0.251-0.531. Fewer intervention participants demonstrated health behavior decline compared with controls. Improved fruit, vegetable, and fat consumption (P<.01) but not exercise were observed in those receiving messages, as compared with controls.
Conclusions: A text messaging intervention was feasible and showed initial evidence of effectiveness in improving diabetes-related health behaviors, demonstrating the potential to facilitate population-level behavior change in a low/middle income country.
Trial registration: Australian New Zealand Clinical Trials Registry (ACTRN): 12615000423516; https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=367946&isReview=true (Archived by WebCite at http://www.webcitation.org/6j5ptaJgF).
Keywords: diabetes; health promotion; mHealth.
Conflict of interest statement
Conflicts of Interest: This study was directed by Arogya World, which received funding support from Aetna International, Lifescan Inc. (a Johnson & Johnson company), and MSD India. The funding sources had no involvement in the conduct of the study, writing of the manuscript, or decision to submit for publication. The corresponding author constructed the manuscript, had final responsibility for the decision to submit, and had full access to all the data in the study.
Linelle Blais received compensation as part of a contract with Arogya World to write the text messages used in this study.
Figures

References
-
- Kaplan WA. Can the ubiquitous power of mobile phones be used to improve health outcomes in developing countries? Global Health. 2006;2:9. doi: 10.1186/1744-8603-2-9. http://www.globalizationandhealth.com/content/2//9 1744-8603-2-9 - DOI - PMC - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
