

Delayed seizures after intracerebral haemorrhage
- PMID: 27497491
- PMCID: PMC5035821
- DOI: 10.1093/brain/aww199
Delayed seizures after intracerebral haemorrhage
Abstract
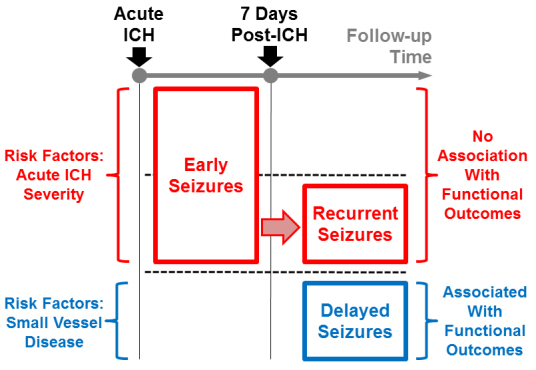
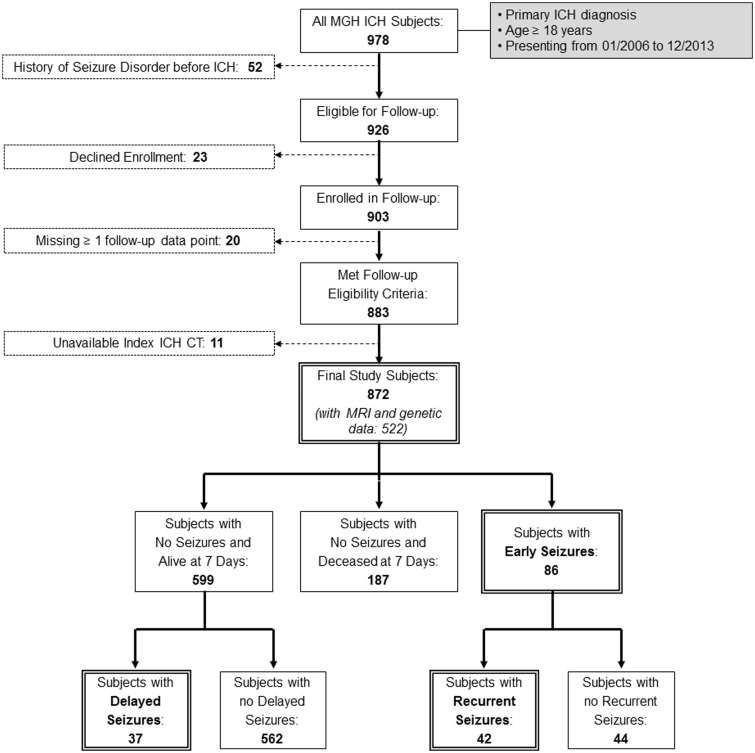
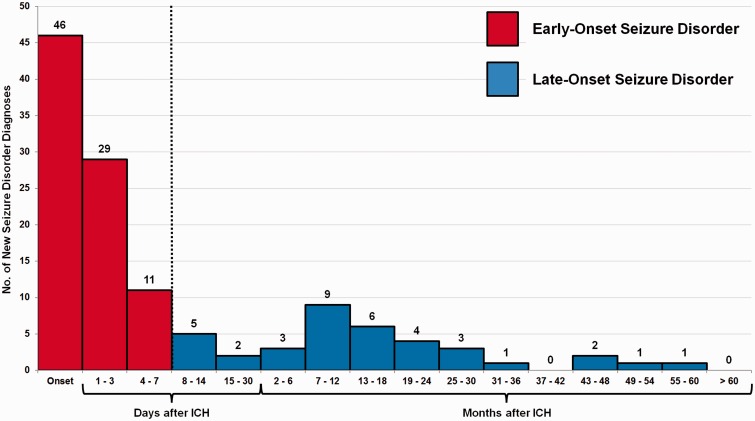
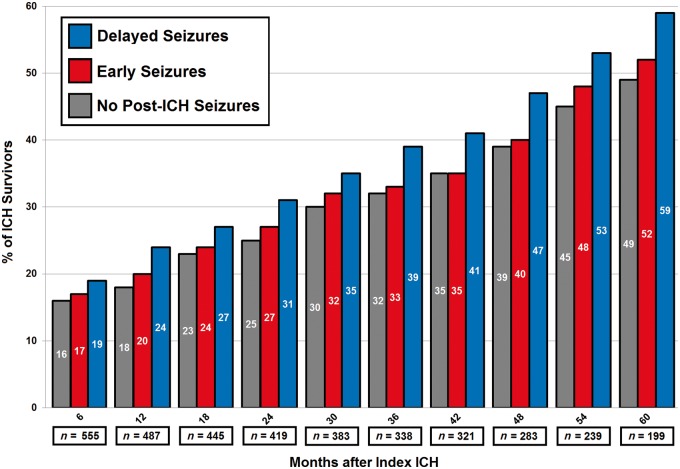
Late seizures after intracerebral haemorrhage occur after the initial acute haemorrhagic insult subsides, and represent one of its most feared long-term sequelae. Both susceptibility to late seizures and their functional impact remain poorly characterized. We sought to: (i) compare patients with new-onset late seizures (i.e. delayed seizures), with those who experienced a recurrent late seizure following an immediately post-haemorrhagic seizure; and (ii) investigate the effect of late seizures on long-term functional performance after intracerebral haemorrhage. We performed prospective longitudinal follow-up of consecutive intracerebral haemorrhage survivors presenting to a single tertiary care centre. We tested for association with seizures the following neuroimaging and genetic markers of cerebral small vessel disease: APOE variants ε2/ε4, computer tomography-defined white matter disease, magnetic resonance imaging-defined white matter hyperintensities volume and cerebral microbleeds. Cognitive performance was measured using the Modified Telephone Interview for Cognitive Status, and functional performance using structured questionnaires obtained every 6 months. We performed time-to-event analysis using separate Cox models for risk to develop delayed and recurrent seizures, as well as for functional decline risk (mortality, incident dementia, and loss of functional independence) after intracerebral haemorrhage. A total of 872 survivors of intracerebral haemorrhage were enrolled and followed for a median of 3.9 years. Early seizure developed in 86 patients, 42 of whom went on to experience recurrent seizures. Admission Glasgow Coma Scale, increasing haematoma volume and cortical involvement were associated with recurrent seizure risk (all P < 0.01). Recurrent seizures were not associated with long-term functional outcome (P = 0.67). Delayed seizures occurred in 37 patients, corresponding to an estimated incidence of 0.8% per year (95% confidence interval 0.5-1.2%). Factors associated with delayed seizures included cortical involvement on index haemorrhage (hazard ratio 1.63, P = 0.036), pre-haemorrhage dementia (hazard ratio 1.36, P = 0.044), history of multiple prior lobar haemorrhages (hazard ratio 2.50, P = 0.038), exclusively lobar microbleeds (hazard ratio 2.22, P = 0.008) and presence of ≥ 1 APOE ε4 copies (hazard ratio 1.95, P = 0.020). Delayed seizures were associated with worse long-term functional outcome (hazard ratio 1.83, P = 0.005), but the association was removed by adjusting for neuroimaging and genetic markers of cerebral small vessel disease. Delayed seizures after intracerebral haemorrhage are associated with different risk factors, when compared to recurrent seizures. They are also associated with worse functional outcome, but this finding appears to be related to underlying small vessel disease. Further investigations into the connections between small vessel disease and delayed seizures are warranted.
Keywords: epilepsy; intracerebral haemorrhage; seizure.
© The Author (2016). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Delayed Seizures and Poor Functional Outcome After Intracranial Hemorrhage Is the Fate of Patients with a Poor Underlying Substrate, Say the Intensivists.Epilepsy Curr. 2017 Mar-Apr;17(2):101-102. doi: 10.5698/1535-7511.17.2.101. Epilepsy Curr. 2017. PMID: 28491000 Free PMC article. No abstract available.
References
-
- Badjatia N, Rosand J. Intracerebral hemorrhage. Neurologist 2005; 11: 311–24. - PubMed
-
- Barber M, Stott DJ. Validity of the Telephone Interview for Cognitive Status (TICS) in post-stroke subjects. Int J Geriatr Psychiatry 2004; 19: 75–9. - PubMed
-
- Beghi E, Carpio A, Forsgren L, Hesdorffer DC, Malmgren K, Sander JW, et al. Recommendation for a definition of acute symptomatic seizure. Epilepsia 2010; 51: 671–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
