

Bowel obstruction and perforation due to a large gallstone. A case report
- PMID: 27497941
- PMCID: PMC4975710
- DOI: 10.1016/j.ijscr.2016.07.050
Bowel obstruction and perforation due to a large gallstone. A case report
Abstract
Introduction: Gallstone bowel obstruction is a rare form of mechanical ileus usually presenting in elderly patients, and is associated with chronic or acute cholecystitis episodes.
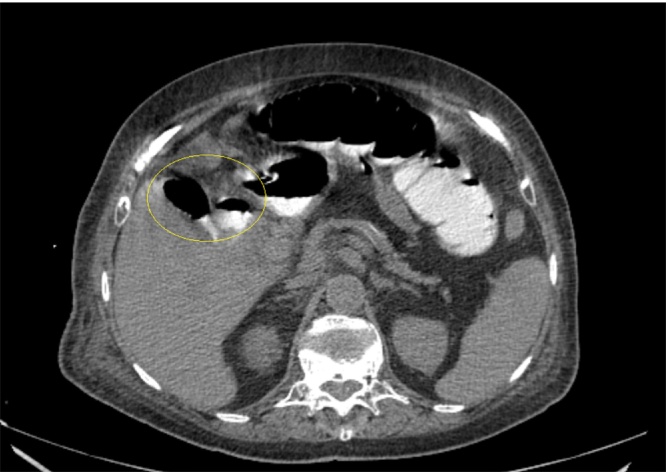
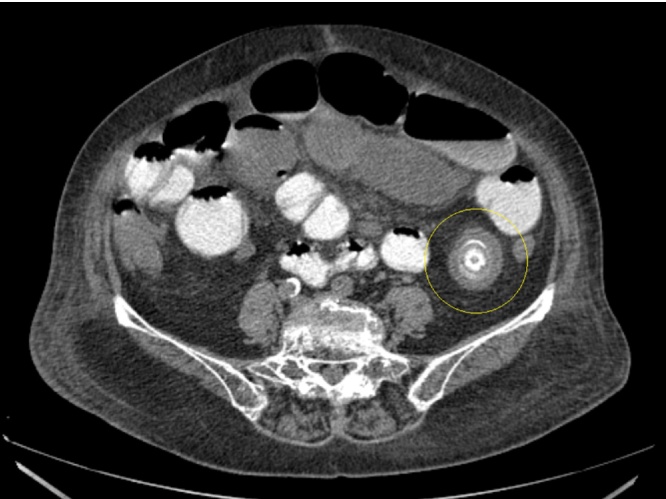
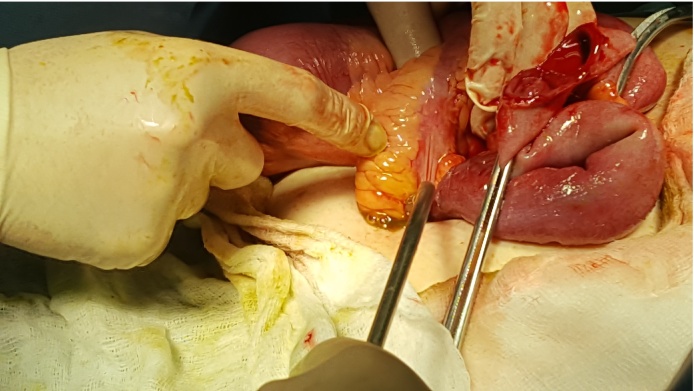
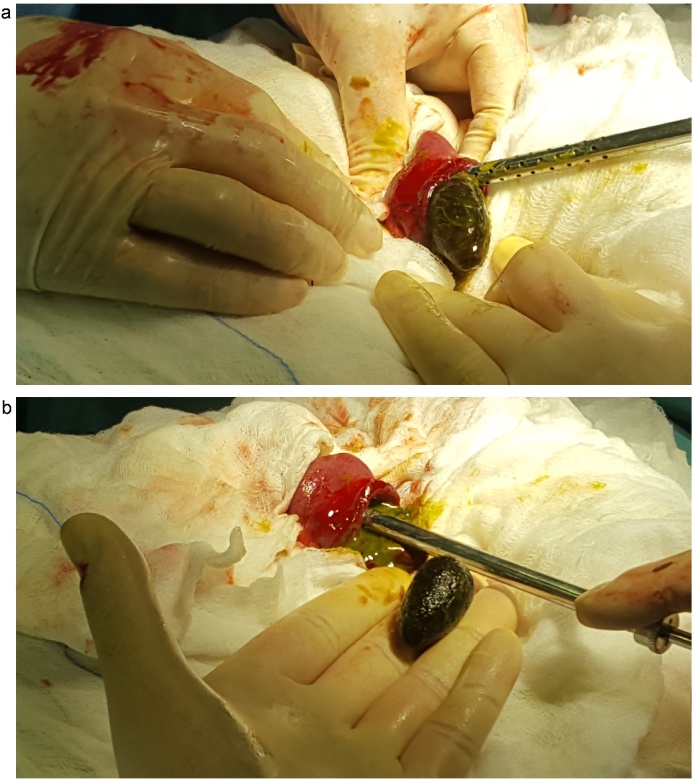
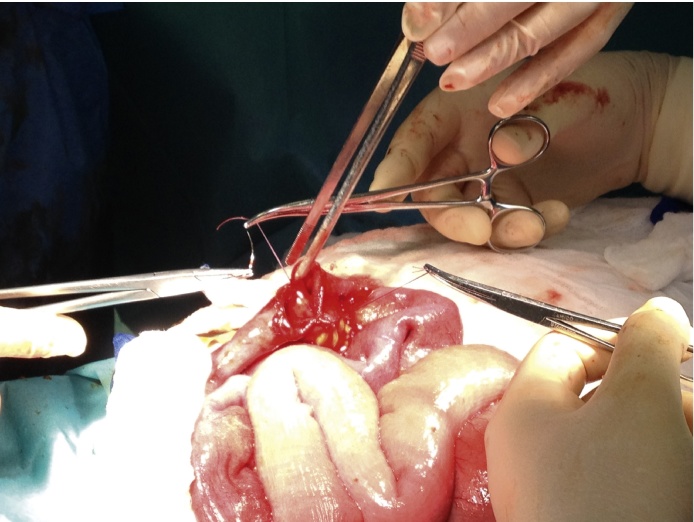
Case presentation: We present the case of an 80year old female with abdominal pain, inability to defecate and recurrent episodes of diarrhea for the past 8 months. CT examination uncovered a cholecystoduodenal fistula along with gas in the gall bladder and the presence of a ≥2cm gallstone inside the small bowel lumen causing obstruction. Patient was admitted to the operating room, where a 3.2cm gallstone was located in the terminal ileus. A rupture was found in the antimesenteric part of a discolored small bowel segment, approximately 60cm from the ileocaecal valve, through which the gallstone was recovered. The bowel regained its peristalsis, and the rupture was debrided and sutured. Patient was discharged uneventfully on the 6th postoperative day.
Discussion: Gallstone ileus is caused due to the impaction of a gallstone inside the bowel lumen. It usually passes through a fistula connecting the gallstone with the gastrointestinal tract. It can present with nonspecific or acute abdominal symptoms. CT usually confirms the diagnosis, while there are a number of treatment options; conservative, minimal invasive and surgical. Our patient was successfully relieved of the obstruction through recovery of the gallstone using open surgery, with no repair of the fistula.
Conclussion: Although rare, gallstones must be suspected as a possible cause of bowel obstruction, especially in elderly patients reporting biliary symptoms.
Keywords: Biliogastric fistula; Case report; Gallstone bowel obstruction; Gallstone ileus; Rigler’s triad.
Copyright © 2016 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures


References
-
- Ayantunde A.A., Agrawal A. Gallstone ileus: diagnosis and management. World J. Surg. 2007;31(6):1292–1297. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
