

Rapid and reliable diagnosis of Wilson disease using X-ray fluorescence
- PMID: 27499926
- PMCID: PMC4958738
- DOI: 10.1002/cjp2.48
Rapid and reliable diagnosis of Wilson disease using X-ray fluorescence
Abstract
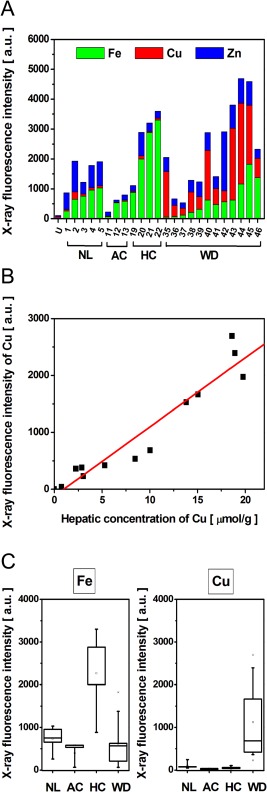
Wilson's disease (WD) is a rare autosomal recessive disease due to mutations of the gene encoding the copper-transporter ATP7B. The diagnosis is hampered by the variability of symptoms induced by copper accumulation, the inconstancy of the pathognomonic signs and the absence of a reliable diagnostic test. We investigated the diagnostic potential of X-ray fluorescence (XRF) that allows quantitative analysis of multiple elements. Studies were performed on animal models using Wistar rats (n = 10) and Long Evans Cinnamon (LEC) rats (n = 11), and on human samples including normal livers (n = 10), alcohol cirrhosis (n = 8), haemochromatosis (n = 10), cholestasis (n = 6) and WD (n = 22). XRF experiments were first performed using synchrotron radiation to address the elemental composition at the cellular level. High-resolution mapping of tissue sections allowed measurement of the intensity and the distribution of copper, iron and zinc while preserving the morphology. Investigations were further conducted using a laboratory X-ray source for irradiating whole pieces of tissue. The sensitivity of XRF was highlighted by the discrimination of LEC rats from wild type even under a regimen using copper deficient food. XRF on whole formalin-fixed paraffin embedded needle biopsies allowed profiling of the elements in a few minutes. The intensity of copper related to iron and zinc significantly discriminated WD from other genetic or chronic liver diseases with 97.6% specificity and 100% sensitivity. This study established a definite diagnosis of Wilson's disease based on XRF. This rapid and versatile method can be easily implemented in a clinical setting.
Keywords: Wilson disease; X‐ray fluorescence spectroscopy; copper; diagnosis.
Figures




References
-
- Tao TY, Gitlin JD. Hepatic copper metabolism: insights from genetic disease. Hepatology 2003; 37: 1241–1247. - PubMed
-
- Ala A, Walker AP, Ashkan K, et al Wilson's disease. Lancet 2007; 369: 397–408. - PubMed
-
- Dziezyc K, Litwin T, Chabik G, et al Families with Wilson's disease in subsequent generations: clinical and genetic analysis. Mov Disord 2014; 29: 1828–1832. - PubMed
-
- Schilsky M, Tavill AS. Wilson disease In Disease of the Liver 2003 (9th edn). Lippicott Williams & Wilkins: Philadelphia, 2003; 1169–1186.
LinkOut - more resources
Full Text Sources
Other Literature Sources
