

Dural repair using autologous fat: Our experience and review of the literature
- PMID: 27500007
- PMCID: PMC4960926
- DOI: 10.4103/2152-7806.185777
Dural repair using autologous fat: Our experience and review of the literature
Abstract
Background: Various materials have been proposed to obliterate dead spaces and to reconstruct dural defects during a neurosurgical approach. This study describes our technique of using the abdominal autologous fat graft and evaluates the complications and characteristics related to the use of this tissue during cranial procedures.
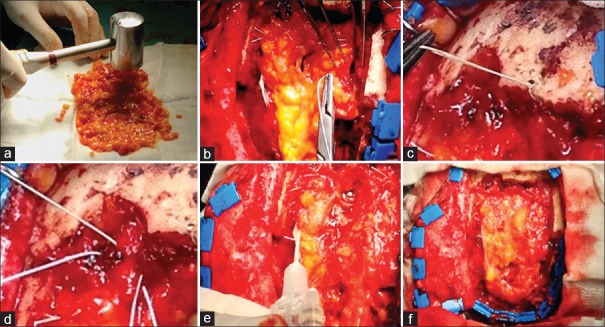
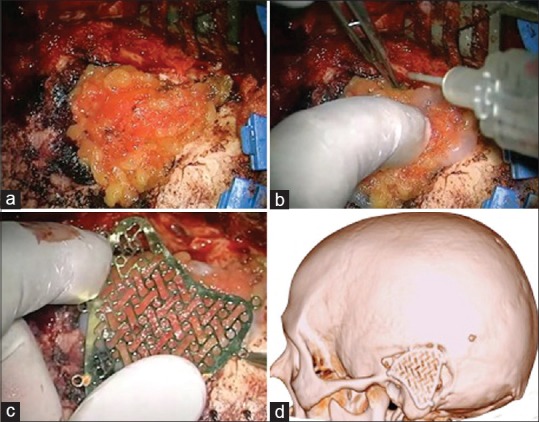
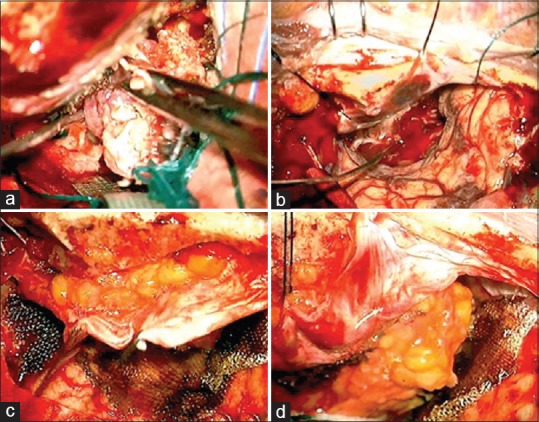
Methods: Autologous fat grafts were used in 296 patients with basicranial and convexity extraaxial tumors from April 2005 to January 2015. The adipose tissue was removed from the paraumbilical abdominal region and was transformed into a thin foil. When possible, a watertight suture was made between the dural or bone edge with a fat graft. We always used fibrin glue to reinforce the dural closure.
Results: Complications occurred between 2 days and 1 year following procedure. Cerebrospinal fluid leaks were found in 11 cases. No case of mortality, pseudomeningoceles, fistula, infections, bacterial meningitides, or lipoid meningitides was reported. No patient required removal of the graft. No adhesion was observed between the brain and the autologous fat. Other fat-related complications observed were 2 cases of fat necrosis in the abdomen and 2 cases of abdominal hemorrhage.
Conclusion: The technique of harvesting and applying fat grafts is fairly simple, although it must be performed meticulously to be effective. Our experience has led us to believe that the use of fat grafts presents low morbidity and mortality. However, a neurosurgeon should never forget the possible late or early complications related to the use of fat grafts.
Keywords: Autologous fat graft; dural repair; dural substitute; watertight suture.
Figures
References
-
- Barth M, Tuettenberg J, Thomé C, Weiss C, Vajkoczy P, Schmiedek P. Watertight dural closure: Is it necessary. A prospective randomized trial in patients with supratentorial craniotomies? Neurosurgery. 2008 Oct;63(4 Suppl 2):S352–8. - PubMed
-
- Black P. Cerebrospinal fluid leaks following spinal or posterior fossa surgery: Use of fat grafts for prevention and repair. Neurosurg Focus. 2000;9:e4. - PubMed
-
- Carvalho GA, Cervio A, Matthies C, Samii M. Subarachnoid fat dissemination after resection of a cerebellopontine angle dysontogenic cyst: Case report and review of the literature. Neurosurgery. 2000;47:760–3. - PubMed
-
- Ferroli P, Acerbi F, Broggi M, Schiariti M, Albanese E, Tringali G, et al. A novel impermeable adhesive membrane to reinforce dural closure: A preliminary retrospective study on 119 consecutive high-risk patients. World Neurosurg. 2013;79:551–7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
