

Pathology of coronary atherosclerosis and thrombosis
- PMID: 27500096
- PMCID: PMC4960071
- DOI: 10.21037/cdt.2016.06.01
Pathology of coronary atherosclerosis and thrombosis
Abstract
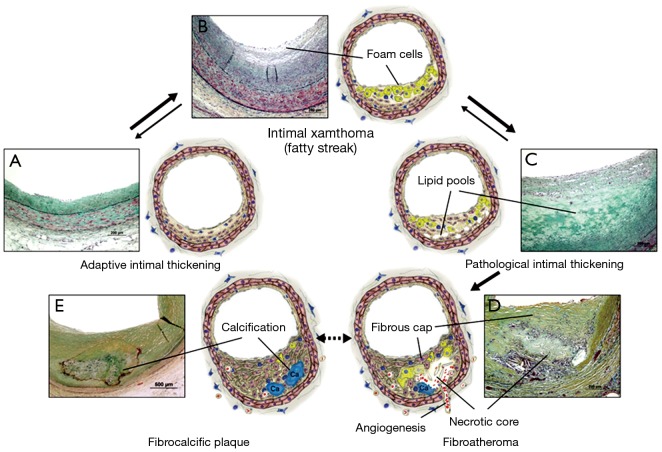
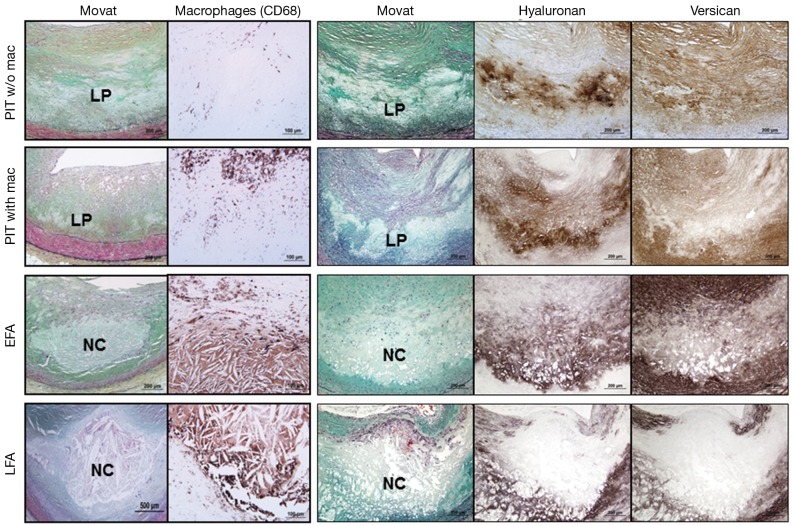
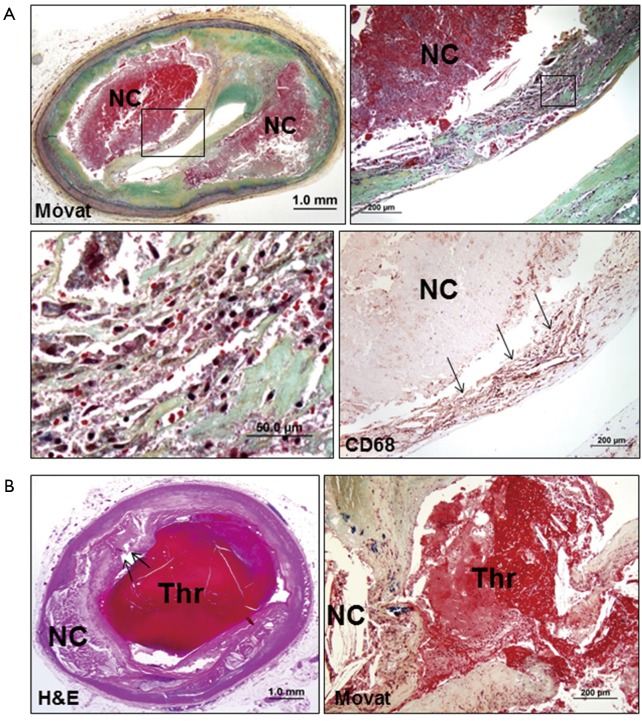
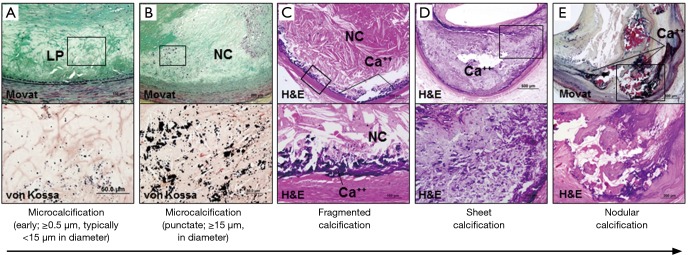
The process of early atherosclerotic plaque progression is characterized by the development of pathologic intimal thickening (PIT) with lipid pool that may transform into the necrotic core to form fibroatheroma, where infiltration of foamy macrophages plays a crucial role. The expansion of the necrotic core is also attributable to intraplaque hemorrhage. Thin-cap fibroatheroma (TCFA) is characterized by a relatively large necrotic core with an overlying thin fibrous cap measuring <65 µm typically containing numerous macrophages, and is considered to be the precursor lesion of plaque rupture which is the most common cause of coronary thrombosis. The second common cause of acute thrombosis is plaque erosion, while calcified nodules is known to be the least frequent cause of coronary thrombosis. Coronary thrombosis can occur without symptoms to form healed lesions, which contributes to an increase in plaque burden and luminal narrowing. The process of plaque progression is generally accompanied by the progression of calcification. An understanding of the histomorphological characteristics of coronary plaques should provide important insights into the pathogenesis, diagnosis, and treatment of atherosclerotic coronary disease for both basic and clinical researchers as well as for clinicians.
Keywords: Atherosclerosis; coronary disease; pathology; thrombosis.
Conflict of interest statement
Figures

References
-
- Stary HC, Chandler AB, Glagov S, et al. A definition of initial, fatty streak, and intermediate lesions of atherosclerosis. A report from the committee on vascular lesions of the council on arteriosclerosis, american heart association. Circulation 1994;89:2462-78. 10.1161/01.CIR.89.5.2462 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous