

Epstein-Barr Virus-Positive Posttransplant Lymphoproliferative Disease After Solid Organ Transplantation: Pathogenesis, Clinical Manifestations, Diagnosis, and Management
- PMID: 27500242
- PMCID: PMC4946499
- DOI: 10.1097/TXD.0000000000000557
Epstein-Barr Virus-Positive Posttransplant Lymphoproliferative Disease After Solid Organ Transplantation: Pathogenesis, Clinical Manifestations, Diagnosis, and Management
Abstract
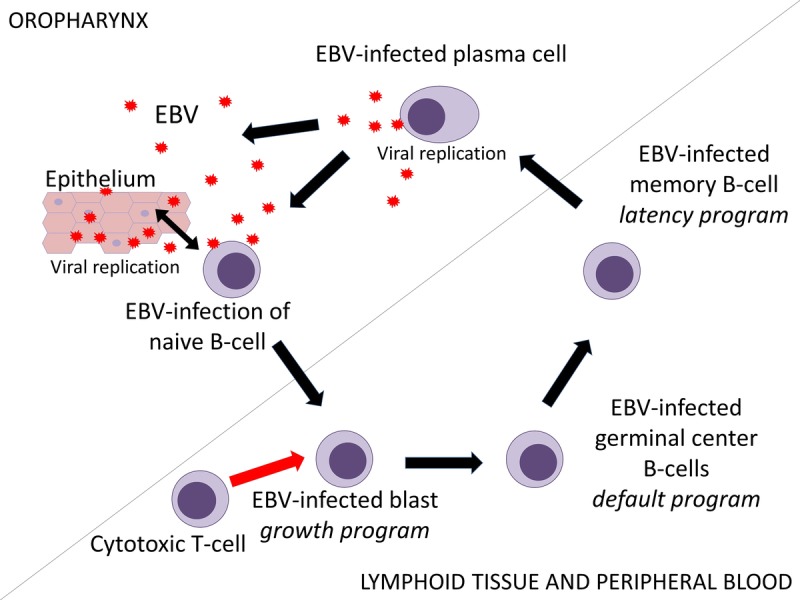
Posttransplant lymphoproliferative disease (PTLD) is a potentially fatal complication after (solid organ) transplantation, which is highly associated with Epstein-Barr virus (EBV). The EBV-specific cytotoxic T cell response that is essential in controlling the virus in healthy individuals is suppressed in transplant recipients using immunosuppressive drugs. A primary EBV infection in EBV-seronegative patients receiving an EBV-seropositive donor organ or a reactivation in those who are already latently infected pretransplantation can lead to uninhibited growth of EBV-infected B cells and subsequently to PTLD. Effective preventive strategies, such as vaccines and antiviral agents, are lacking. Because not every transplant recipient with increasing EBV viral load develops PTLD, it is hard to decide how intensively these patients should be monitored and how and when a preemptive intervention should take place. There is a need for other tools to help predict the development of PTLD in patients at risk to make timing and strategy of preemptive intervention easier and more reliable. The cornerstone of the treatment of patients with PTLD is restoring the host's immunity by reduction of immunosuppressive drug therapy. American and British guidelines recommend to add rituximab monotherapy or rituximab in combination with cyclophosphamide, doxorubicin, vincristine, and prednisolone, depending on histology and clinical characteristics. Although response to these therapies is good, toxicity is a problem, and PTLD still has a relatively high mortality rate. An evolving therapy, especially in PTLD occurring in allogeneic stem cell transplantation, is restoring the host's immune response with infusion of EBV-specific cytotoxic T cells. This may also play a role in the future in both prevention and treatment of PTLD in SOT.
Figures
References
-
- Cohen JI. Epstein-Barr virus infection. N Engl J Med. 2000; 343: 481– 492. - PubMed
-
- Tsurumi T, Fujita M, Kudoh A. Latent and lytic Epstein-Barr virus replication strategies. Rev Med Virol. 2005; 15: 3– 15. - PubMed
-
- Thorley-Lawson DA, Gross A. Persistence of the Epstein-Barr virus and the origins of associated lymphomas. N Engl J Med. 2004; 350: 1328– 1337. - PubMed
-
- Nourse JP, Jones K, Gandhi MK. Epstein-Barr virus-related post-transplant lymphoproliferative disorders: pathogenetic insights for targeted therapy. Am J Transplant. 2011; 11: 888– 895. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
