

Deep Vein Thrombosis and Pulmonary Embolism in Liver Transplant Patients: Risks and Prevention
- PMID: 27500259
- PMCID: PMC4946512
- DOI: 10.1097/TXD.0000000000000578
Deep Vein Thrombosis and Pulmonary Embolism in Liver Transplant Patients: Risks and Prevention
Abstract
Deep vein thrombosis (DVT) and pulmonary embolism (PE) are surgical complications estimated to occur in 5% to 10% of patients. There are limited data regarding DVT/PE in the early postoperative period in liver transplant patients. The aim of this study is to determine risk factors that influence the incidence of DVT/PE and the effectiveness of prophylaxis.
Methods: We reviewed the records of 999 patients who underwent initial liver transplant between January 2000 and June 2012 at Henry Ford Hospital. In 2011, a standardized prophylactic regimen using subcutaneous (SQ) heparin was initiated. All patients that developed either upper/lower extremity DVT or PE within the first 30 days of transplant formed the cohort of this study.
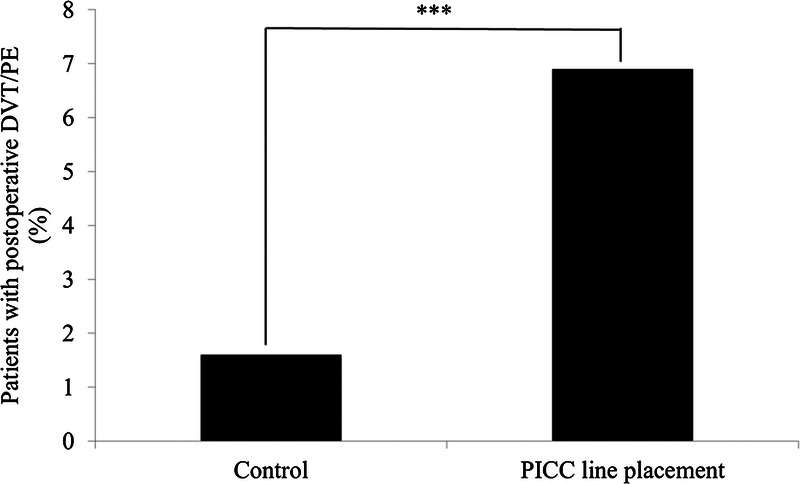
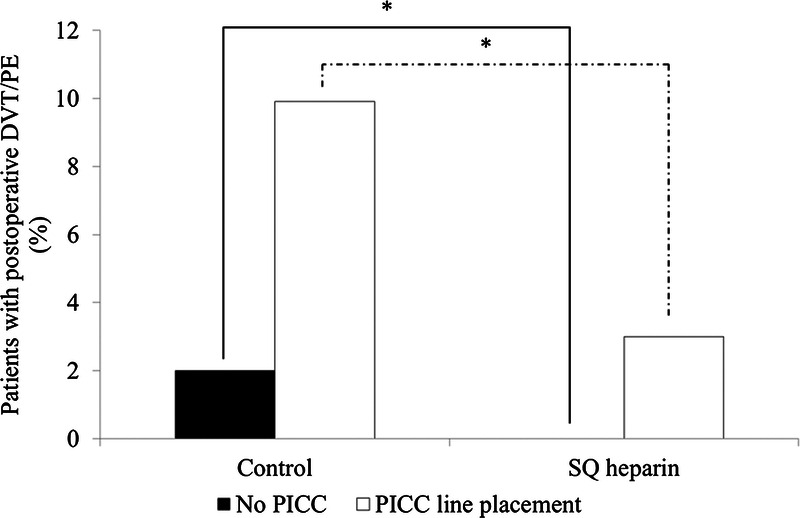
Results: On multivariate analysis, only peripherally inserted central catheter (PICC) placement and SQ heparin were associated with DVT/PE. In patients receiving heparin, 3 (1.0%) had DVT/PE versus 25 (3.5%) who did not receive heparin (P = 0.03). Sixteen (6.9%) patients that had a PICC developed DVT/PE compared with 12 (1.6%) patients without a PICC (P < 0.001). In the heparin group, DVT/PE with PICC was reduced to 3 (3.0%) versus 13 (9.9%) in those with a PICC and did not receive heparin (P = 0.03). Mean time from transplant to DVT/PE diagnosis was 12.3 days. Length of hospitalization was significantly longer in patients who developed DVT/PE (18.5 vs 10.0 days, P < 0.001).
Conclusions: In this study, we demonstrated that PICC placement significantly increases the likelihood of DVT/PE in liver transplant recipients. Prophylactic SQ heparin effectively reduced DVT/PE events in this patient population.
Conflict of interest statement
The authors declare no funding or conflicts of interest.
Figures
Similar articles
-
Risk of deep vein thrombosis and pulmonary embolism after heart transplantation: clinical outcomes comparing upper extremity deep vein thrombosis and lower extremity deep vein thrombosis.Clin Transplant. 2015 Jul;29(7):629-35. doi: 10.1111/ctr.12566. Epub 2015 Jun 16. Clin Transplant. 2015. PMID: 25982188
-
Risk factors for deep vein thrombosis and pulmonary embolism after traumatic injury: A competing risks analysis.J Trauma Acute Care Surg. 2017 Dec;83(6):1154-1160. doi: 10.1097/TA.0000000000001652. J Trauma Acute Care Surg. 2017. PMID: 28697017
-
Venous thromboembolism: deep venous thrombosis and pulmonary embolism in a neurosurgical population.J Neurosurg. 2011 Jan;114(1):40-6. doi: 10.3171/2010.8.JNS10332. Epub 2010 Sep 3. J Neurosurg. 2011. PMID: 20815694
-
Predictive risk factors of venous thromboembolism (VTE) associated with peripherally inserted central catheters (PICC) in ambulant solid cancer patients: retrospective single Centre cohort study.Thromb J. 2019 Jan 25;17:2. doi: 10.1186/s12959-019-0191-y. eCollection 2019. Thromb J. 2019. PMID: 30697126 Free PMC article. Review.
-
Peripherally Inserted Central Catheter-associated Deep Vein Thrombosis: A Narrative Review.Am J Med. 2015 Jul;128(7):722-38. doi: 10.1016/j.amjmed.2015.01.027. Epub 2015 Feb 16. Am J Med. 2015. PMID: 25697969 Review.
Cited by
-
What is the optimal management of thromboprophylaxis after liver transplantation regarding prevention of bleeding, hepatic artery, or portal vein thrombosis? A systematic review of the literature and expert panel recommendations.Clin Transplant. 2022 Oct;36(10):e14629. doi: 10.1111/ctr.14629. Clin Transplant. 2022. PMID: 35240723 Free PMC article.
-
Development and validation of a predictive nomogram for venous thromboembolism in adult patients undergoing orthotopic liver transplantation.Chin Med J (Engl). 2024 Sep 20;137(18):2254-2256. doi: 10.1097/CM9.0000000000003272. Epub 2024 Aug 27. Chin Med J (Engl). 2024. PMID: 39187965 Free PMC article. No abstract available.
-
Vascular boot warming improves clinical outcomes of patients with deep vein thrombosis in lower extremities.Am J Transl Res. 2021 Apr 15;13(4):3800-3805. eCollection 2021. Am J Transl Res. 2021. PMID: 34017568 Free PMC article.
-
Perioperative thromboprophylaxis in liver transplant patients.World J Gastroenterol. 2018 Jul 21;24(27):2931-2948. doi: 10.3748/wjg.v24.i27.2931. World J Gastroenterol. 2018. PMID: 30038462 Free PMC article. Review.
-
Pre-Transplant Factors Influencing Rates of Hepatocellular Carcinoma Recurrence in Liver Transplant Recipients.Gastroenterology Res. 2021 Jun;14(3):190-193. doi: 10.14740/gr1402. Epub 2021 Jun 19. Gastroenterology Res. 2021. PMID: 34267835 Free PMC article.
References
-
- Anderson FA, Wheeler HB. Venous thromboembolism. Risk factors and prophylaxis. Clin Chest Med. 1995; 16: 235– 251. - PubMed
-
- Cushman M, Tsai AW, White RH, et al. Deep vein thrombosis and pulmonary embolism in two cohorts: the longitudinal investigation of thromboembolism etiology. Am J Med. 2004; 117: 19– 25. - PubMed
-
- Heit JA, Silverstein MD, Mohr DN, et al. Predictors of survival after deep vein thrombosis and pulmonary embolism: a population-based, cohort study. Arch Intern Med. 1999; 159: 445– 453. - PubMed
-
- Agnelli G. Prevention of venous thromboembolism in surgical patients. Circulation. 2004; 110(24 Suppl 1): IV4– 12. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
