

Differences in Serum Human Chorionic Gonadotropin Rise in Early Pregnancy by Race and Value at Presentation
- PMID: 27500326
- PMCID: PMC4993627
- DOI: 10.1097/AOG.0000000000001568
Differences in Serum Human Chorionic Gonadotropin Rise in Early Pregnancy by Race and Value at Presentation
Abstract
Objective: To assess whether variation in serum human chorionic gonadotropin (hCG) measures, used to assess early gestation viability, are associated with differences in clinical presentation and patient factors.
Method: This retrospective cohort study included 285 women with first-trimester pain and bleeding and a pregnancy of unknown location for whom a normal intrauterine pregnancy was ultimately confirmed. Serial samples were collected at three U.S. sites and hCG changes were analyzed for differences by race, ethnicity, and clinical factors. A nonlinear, mixed-effects regression model was used assuming a random subject shift in the time axis.
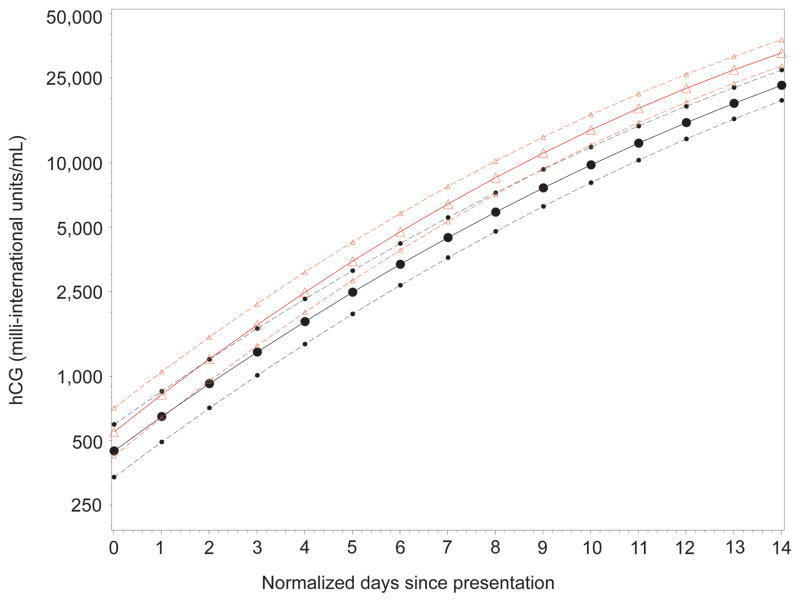
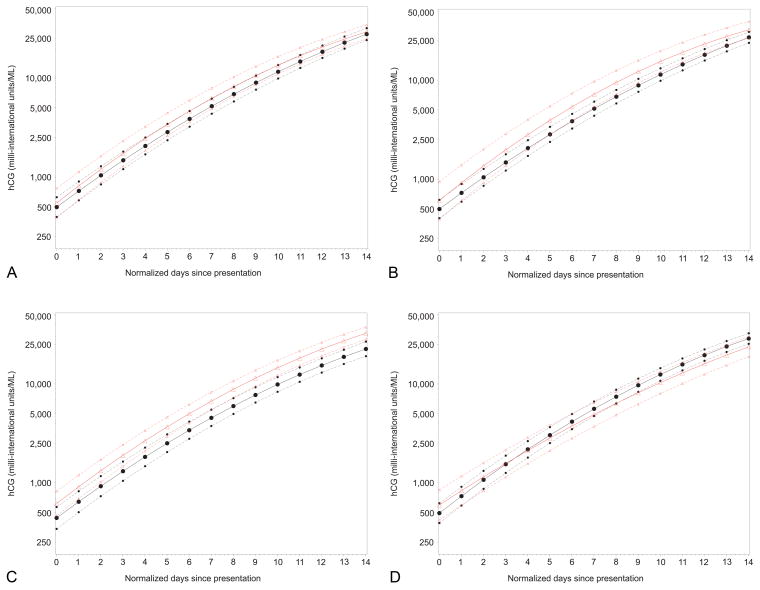
Results: The hCG rise in symptomatic women with ongoing intrauterine pregnancy differs by patient factors and level at presentation. The 2-day minimum (first percentile) rise in hCG was faster when presenting hCG values were low and slower when presenting hCG value was high. African American women had a faster hCG rise (P<.001) compared with non-African American women. Variation in hCG curves was associated with prior miscarriage (P=.014), presentation of bleeding (P<.001), and pain (P=.002). For initial hCG values of less than 1,500, 1,500-3,000 and greater than 3,000 milli-international units/mL, the predicted 2-day minimal (first percentile) rise was 49%, 40%, and 33%, respectively.
Conclusion: The rise of hCG levels in women with viable intrauterine pregnancies and symptoms of potential pregnancy failure varies significantly by initial value. Changes in hCG rise related to race should not affect clinical care. To limit interruption of a potential desired intrauterine pregnancy, a more conservative "cutoff" (slower rise) is needed when hCG values are high.
Clinical trial registration: ClinicalTrials.gov, https://clinicaltrials.gov, NCT00194168.
Figures
References
-
- Shalev E, Yarom I, Bustan M, Weiner E, Ben-Shlomo I. Transvaginal sonography as the ultimate diagnostic tool for the management of ectopic pregnancy: experience with 840 cases. Fertil Steril. 1998;69:62–5. - PubMed
-
- Kadar N, Caldwell BV, Romero R. A method of screening for ectopic pregnancy and its indications. Obstet Gynecol. 1981;58:162–6. - PubMed
-
- Kirk E, Bourne T. Predicting outcomes in pregnancies of unknown location. Womens Health. 2008;4:491–5. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
