

Measuring the Value of a Clinical Practice Guideline for Children With Perforated Appendicitis
- PMID: 27501175
- PMCID: PMC10210014
- DOI: 10.1097/SLA.0000000000001946
Measuring the Value of a Clinical Practice Guideline for Children With Perforated Appendicitis
Abstract
Objective: To determine the incremental cost-effectiveness of a clinical practice guideline (CPG) compared with "usual care" for treatment of perforated appendicitis in children. Secondary objective was to compare cost analyses using hospital accounting system data versus data in the Pediatric Health Information System (PHIS).
Background: Value-based surgical care (outcomes relative to costs) is frequently touted, but outcomes and costs are rarely measured together.
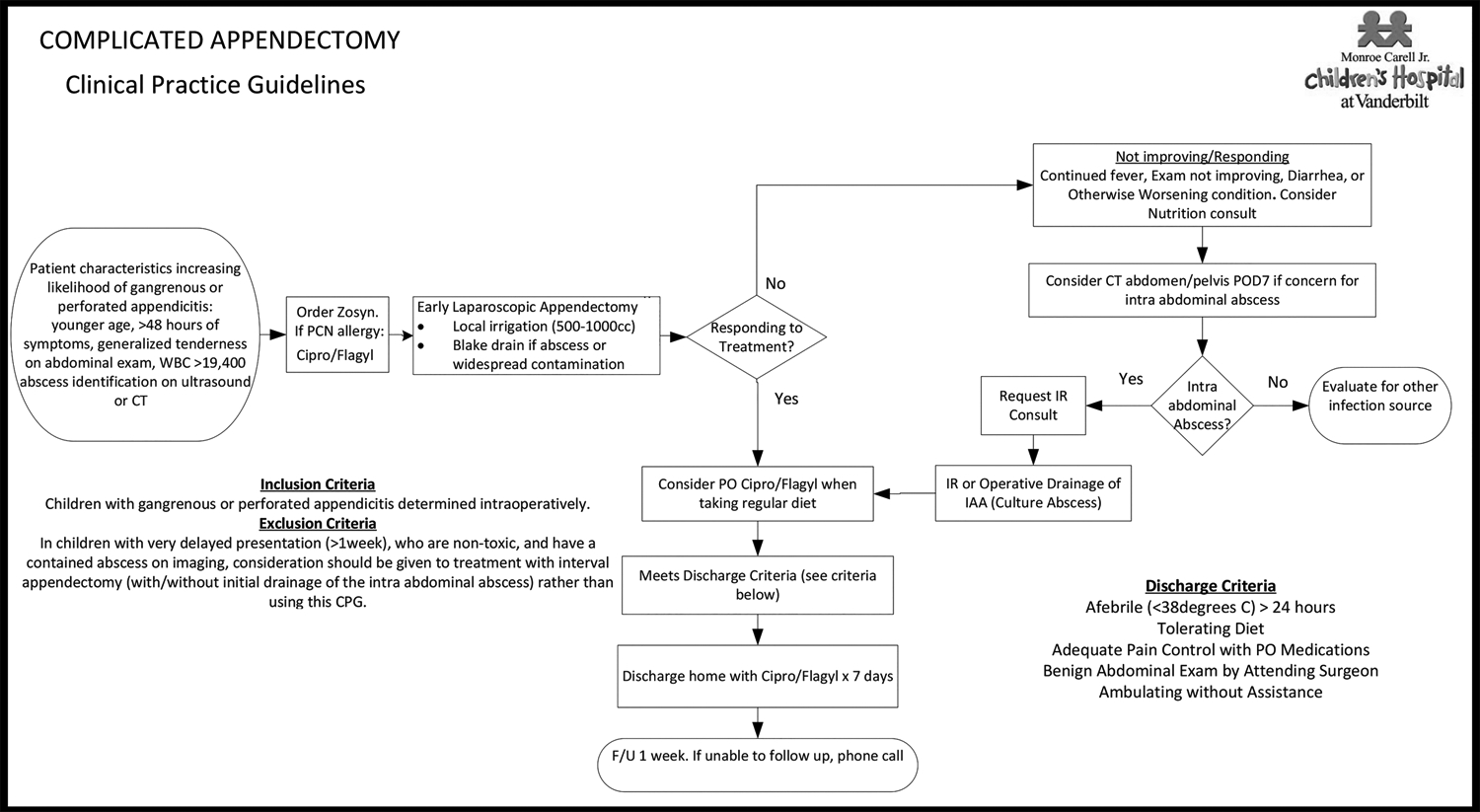
Methods: During an 18-month period, 122 children with perforated appendicitis at a tertiary referral children's hospital were treated using an evidence-based CPG. Clinical outcomes and costs for the CPG cohort were compared with patients in the 30-month period before CPG implementation (n = 191 children).
Results: With CPG-directed care, intra-abdominal abscess rate decreased from 0.24 to 0.10 (adjusted risk ratio 0.44, 95% confidence interval [CI] 0.26-0.75). The rate of any adverse event decreased from 0.30 to 0.23 (adjusted risk ratio 0.82, 95% CI 0.58-1.17). Mean total hospital costs per patient (hospital accounting system) decreased from $16,466 to $10,528 (adjusted absolute difference-$5451, 95% CI -$7755 to -$3147), leading to estimated adjusted total savings of $665,022 during the study period. Costs obtained from the PHIS database also showed reduction with CPG-directed care (-$6669, 95% CI -$8949 to -$4389 per patient). In Bayesian cost-effectiveness analyses, likelihood that CPG was the dominant strategy was 91%.
Conclusions: An evidence-based CPG increased the value of surgical care for children with perforated appendicitis by improving outcomes and lowering costs. Hospital cost accounting data and pre-existing cost data within the PHIS database provided similar results.
Conflict of interest statement
JR Robinson receives salary and tuition support by the 5T15LM007450 training grant from the NIH National Library of Medicine. ZI Willis receives support from the NIH training grant 5 T32 AI095202-02, Childhood Infection Research Program. EBC Avritscher and JE Tyson receive grant support by the Centers for Medicare and Medicaid Services ICMS 331044-03-00 Health Care Innovation Award. EBC Avritscher receives grant support from the Department of Health and Human Services 1P30HS024459-01 Agency for Healthcare Research & Quality Grant.
Figures
References
-
- Porter ME. What is value in health care? N Engl J Med 2010; 363(26):2477–2481. - PubMed
-
- Smoldt RK, Cortese DA. Pay-for-performance or pay for value? Mayo Clin Proc 2007; 82(2):210–213. - PubMed
-
- Cosgrove T. Value-Based Health Care Is Inevitable and That’s Good. Harvard Business Review, 2013.
-
- Burwell SM. Setting value-based payment goals--HHS efforts to improve U.S. health care. N Engl J Med 2015; 372(10):897–899. - PubMed
-
- Imus S. Healthcare cost accounting: 8 strategies to streamline implementation and quickly achieve measurable results. 2014. Accessed February 29, 2016. Available from: http://www.beckershospitalreview.com/finance/healthcare-cost-accounting-....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
