

Survey of the anti-factor IX immunoglobulin profiles in patients with hemophilia B using a fluorescence-based immunoassay
- PMID: 27501440
- PMCID: PMC5083216
- DOI: 10.1111/jth.13438
Survey of the anti-factor IX immunoglobulin profiles in patients with hemophilia B using a fluorescence-based immunoassay
Abstract
Essentials Studies characterizing neutralizing antibodies (inhibitors) in hemophilia B (HB) are lacking. The current study describes anti-factor (F) IX antibody profiles in 37 patients who have HB. Anti-FIX IgG4 levels exhibited a strong positive correlation with Nijmegen-Bethesda results. These data will help to more clearly define, predict, and treat alloantibody formation in HB.
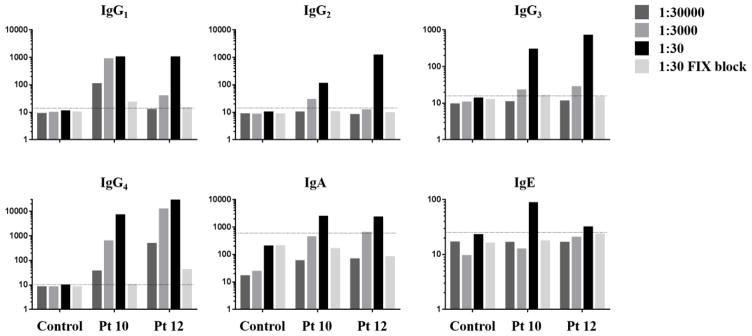
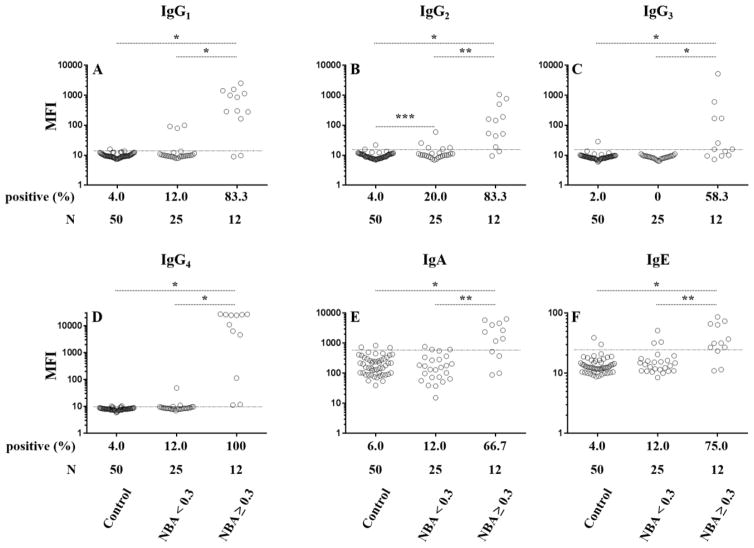
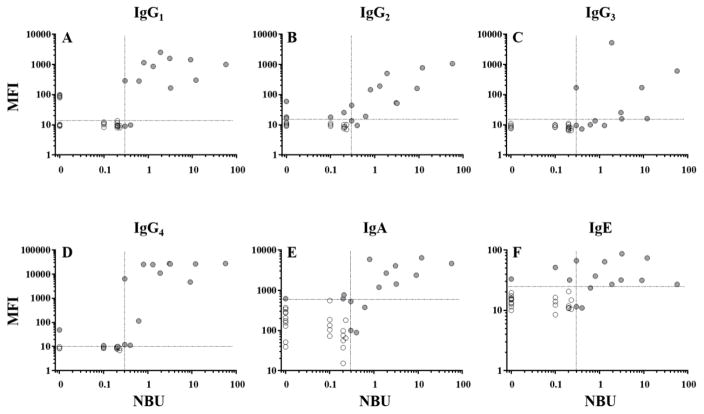
Summary: Background Hemophilia B (HB) is an inherited bleeding disorder caused by the absence or dysfunction of coagulation factor IX (FIX). A subset of patients who have HB develop neutralizing alloantibodies (inhibitors) against FIX after infusion therapy. HB prevalence and the proportion of patients who develop inhibitors are much lower than those for hemophilia A (HA), which makes studies of inhibitors in patients with HB challenging due to the limited availability of samples. As a result, there is a knowledge gap regarding HB inhibitors. Objective Evaluate the largest group of patients with inhibitor-positive HB studied to date to assess the relationship between anti-FIX antibody profiles and inhibitor formation. Methods A fluorescence immunoassay was used to detect anti-FIX antibodies in plasma samples from 37 patients with HB. Results Assessments of antibody profiles showed that anti-FIX IgG1-4 , IgA, and IgE were detected significantly more often in patients with a positive Nijmegen-Bethesda assay (NBA). All NBA-positive samples were positive for IgG4 . Anti-FIX IgG4 demonstrated a strong correlation with the NBA, while correlations were significant, yet more moderate, for anti-FIX IgG1-2 and IgA. Conclusions The anti-FIX antibody profile in HB patients who develop inhibitors is diverse and correlates well with the NBA across immunoglobulin (sub)class, and anti-FIX IgG4 is particularly relevant to functional inhibition. The anti-FIX fluorescence immunoassay may serve as a useful tool to confirm the presence of antibodies in patients who have low positive NBA results and to more clearly define, predict, and treat alloantibody formation against FIX.
Keywords: factor IX; factor IX deficiency; hemophilia B; immunoassay; inherited blood coagulation disorders.
© 2016 International Society on Thrombosis and Haemostasis.
Conflict of interest statement
of Conflict of Interests C. Kempton reports grants from CDC Foundation during the conduct of the study; grants and personal fees from Novo Nordisk, as well as personal fees from Baxalta, Biogen Idec, and CSL Behring outside the submitted work. A. Neff reports grants from CDC Foundation during the conduct of the study; grants from Baxter, Novo Nordisk, and CSL Behring, as well as personal fees from Alexion outside the submitted work. C. Miller reports grants from CDC Foundation during the conduct of the study. A. Dunn reports grants and personal fees from Biogen, Bayer, Baxalta, and CSL Behring; grants from Octopharma, Kedrion, and Novo Nordisk outside the submitted work. S. R. Lentz reports grants from CDC Foundation during the conduct of the study; personal fees from Novo Nordisk outside the submitted work. M. Tarantino reports personal fees and other from Bleeding and Clotting Disorders Institute, Novo Nordisk, Baxalta, Grifols, Amgem, Pfizer, Biogen, HRSA, and CDC Foundation outside the submitted work. A. Escobar reports grants and personal fees from Pfizer, personal fees from Baxalta, Novo Nordisk, Bayer, and CSL Behring outside the submitted work. C. Lessinger reports grants from Baxalta, CSL Behring, and Roche; advisory board participation in Baxalta, Bayer, CSL Behring, Kedrion, Novo Nordisk, Roche, Pfizer, Biogen, and LFB. J. C. Gill reports grants from Centers for Disease Control and Prevention during the conduct of the study; grants and personal fees from CSL Behring Shire and Bayer outside the submitted work. B. M. Wicklund reports grants from CDC Foundation during the conduct of the study; personal fees from Novo Nordisk, Biogen, Baxalta-Shire, Bayer, and Oakstone-EBIX outside the submitted work.
Figures
Similar articles
-
Characterization of the anti-factor VIII immunoglobulin profile in patients with hemophilia A by use of a fluorescence-based immunoassay.J Thromb Haemost. 2015 Jan;13(1):47-53. doi: 10.1111/jth.12768. Epub 2014 Dec 11. J Thromb Haemost. 2015. PMID: 25354263 Free PMC article.
-
Involvement of the IgE-basophil system and mild complement activation in haemophilia B with anti-factor IX neutralizing antibodies and anaphylaxis.Haemophilia. 2017 Jul;23(4):e348-e353. doi: 10.1111/hae.13282. Epub 2017 Jun 8. Haemophilia. 2017. PMID: 28594432
-
Measurement of anti-factor IX IgG subclasses in haemophilia B patients who developed inhibitors with episodes of allergic reactions to factor IX concentrates.Thromb Res. 1996 Aug 15;83(4):279-86. doi: 10.1016/0049-3848(96)00136-3. Thromb Res. 1996. PMID: 8870172
-
Inhibitor antibodies to factor VIII and factor IX: management.Semin Thromb Hemost. 2000;26(2):179-88. doi: 10.1055/s-2000-9821. Semin Thromb Hemost. 2000. PMID: 10919411 Review.
-
Desensitization and immune tolerance induction in children with severe factor IX deficiency; inhibitors and adverse reactions to replacement therapy: a case-report and literature review.Ital J Pediatr. 2015 Feb 19;41:12. doi: 10.1186/s13052-015-0116-8. Ital J Pediatr. 2015. PMID: 25887512 Free PMC article. Review.
Cited by
-
Nonneutralizing antibodies in Nordic persons with moderate hemophilia A and B (the MoHem study).Res Pract Thromb Haemost. 2024 Oct 29;8(8):102611. doi: 10.1016/j.rpth.2024.102611. eCollection 2024 Nov. Res Pract Thromb Haemost. 2024. PMID: 39807249 Free PMC article.
-
Evaluation of CDC's Hemophilia Surveillance Program - Universal Data Collection (1998-2011) and Community Counts (2011-2019), United States.MMWR Surveill Summ. 2020 Sep 4;69(5):1-18. doi: 10.15585/mmwr.ss6905a1. MMWR Surveill Summ. 2020. PMID: 32881847 Free PMC article.
-
Soluble expression of recombinant coagulation factor IX protein using Escherichia coli.Biochem Biophys Rep. 2024 Apr 18;38:101714. doi: 10.1016/j.bbrep.2024.101714. eCollection 2024 Jul. Biochem Biophys Rep. 2024. PMID: 38681671 Free PMC article.
-
Laboratory testing for factor VIII and IX inhibitors in haemophilia: A review.Haemophilia. 2018 Mar;24(2):186-197. doi: 10.1111/hae.13424. Epub 2018 Feb 15. Haemophilia. 2018. PMID: 29446525 Free PMC article. Review.
References
-
- Dimichele D. Inhibitor development in haemophilia B: an orphan disease in need of attention. Br J Haematol. 2007 Aug;138:305–15. - PubMed
-
- Astermark J, Morado M, Rocino A, Van Den Berg HM, von DM, Gringeri A, Mantovani L, Garrido RP, Schiavoni M, Villar A, Windyga J. Current European practice in immune tolerance induction therapy in patients with haemophilia and inhibitors. Haemophilia. 2006 Jul;12:363–71. - PubMed
-
- Benson G, Auerswald G, Elezovic I, Lambert T, Ljung R, Morfini M, Remor E, Salek SZ. Immune tolerance induction in patients with severe hemophilia with inhibitors: expert panel views and recommendations for clinical practice. Eur J Haematol. 2012 May;88:371–9. - PubMed
-
- Warrier I, Ewenstein BM, Koerper MA, Shapiro A, Key N, Dimichele D, Miller RT, Pasi J, Rivard GE, Sommer SS, Katz J, Bergmann F, Ljung R, Petrini P, Lusher JM. Factor IX inhibitors and anaphylaxis in hemophilia B. J Pediatr Hematol Oncol. 1997 Jan;19:23–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
