

Epidemiology and Impact of Campylobacter Infection in Children in 8 Low-Resource Settings: Results From the MAL-ED Study
- PMID: 27501842
- PMCID: PMC5064165
- DOI: 10.1093/cid/ciw542
Epidemiology and Impact of Campylobacter Infection in Children in 8 Low-Resource Settings: Results From the MAL-ED Study
Abstract
Background: Enteropathogen infections have been associated with enteric dysfunction and impaired growth in children in low-resource settings. In a multisite birth cohort study (MAL-ED), we describe the epidemiology and impact of Campylobacter infection in the first 2 years of life.
Methods: Children were actively followed up until 24 months of age. Diarrheal and nondiarrheal stool samples were collected and tested by enzyme immunoassay for Campylobacter Stool and blood samples were assayed for markers of intestinal permeability and inflammation.
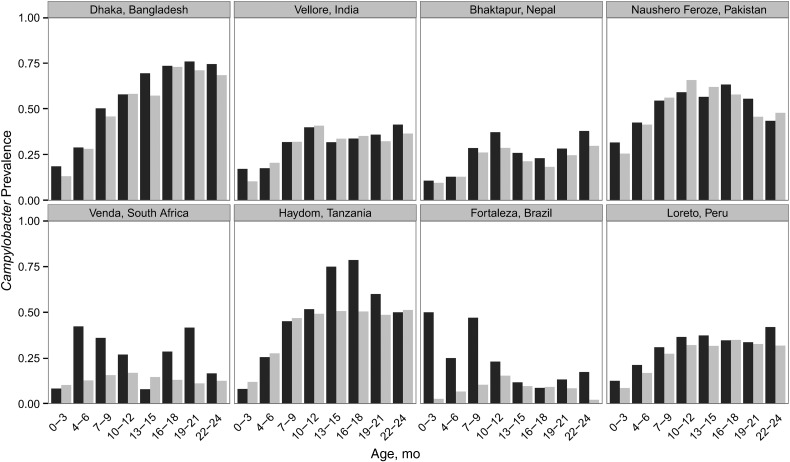
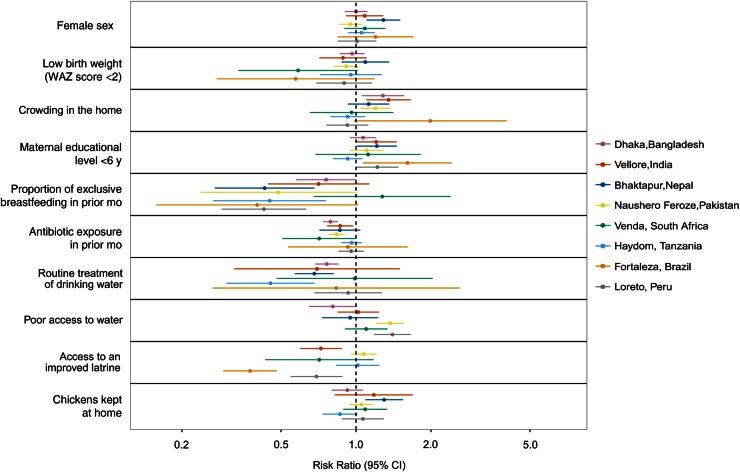
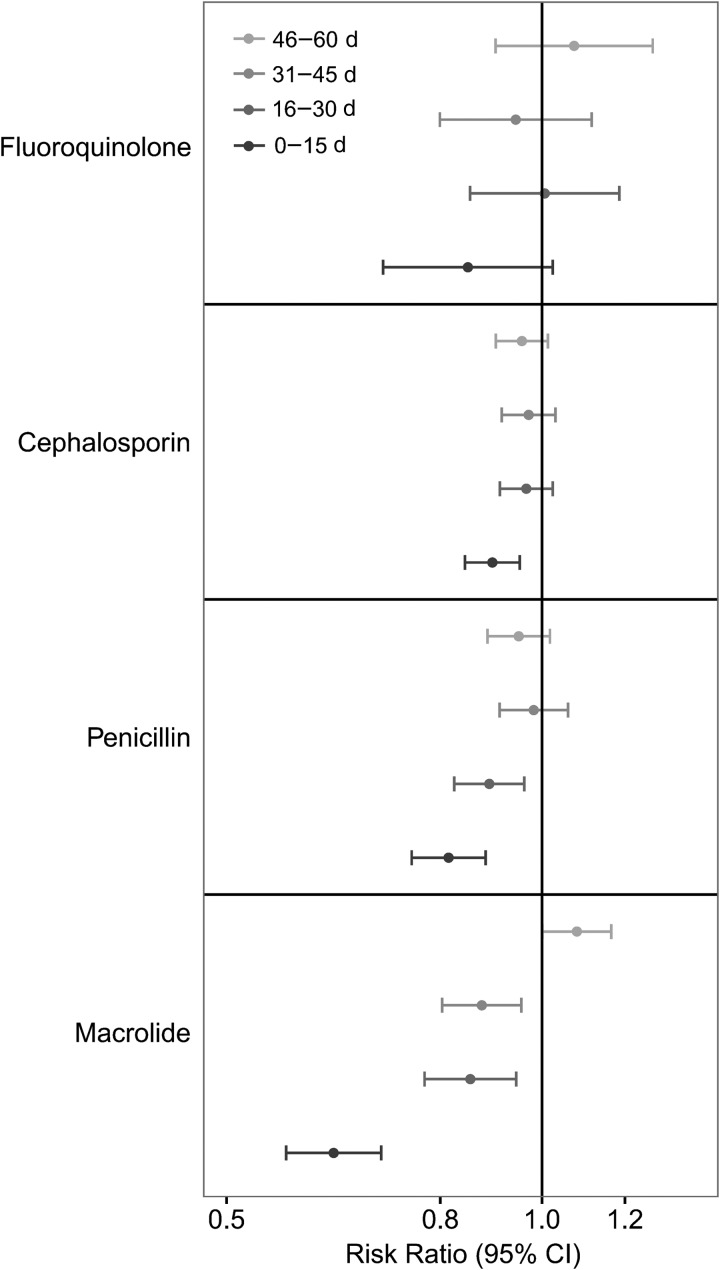
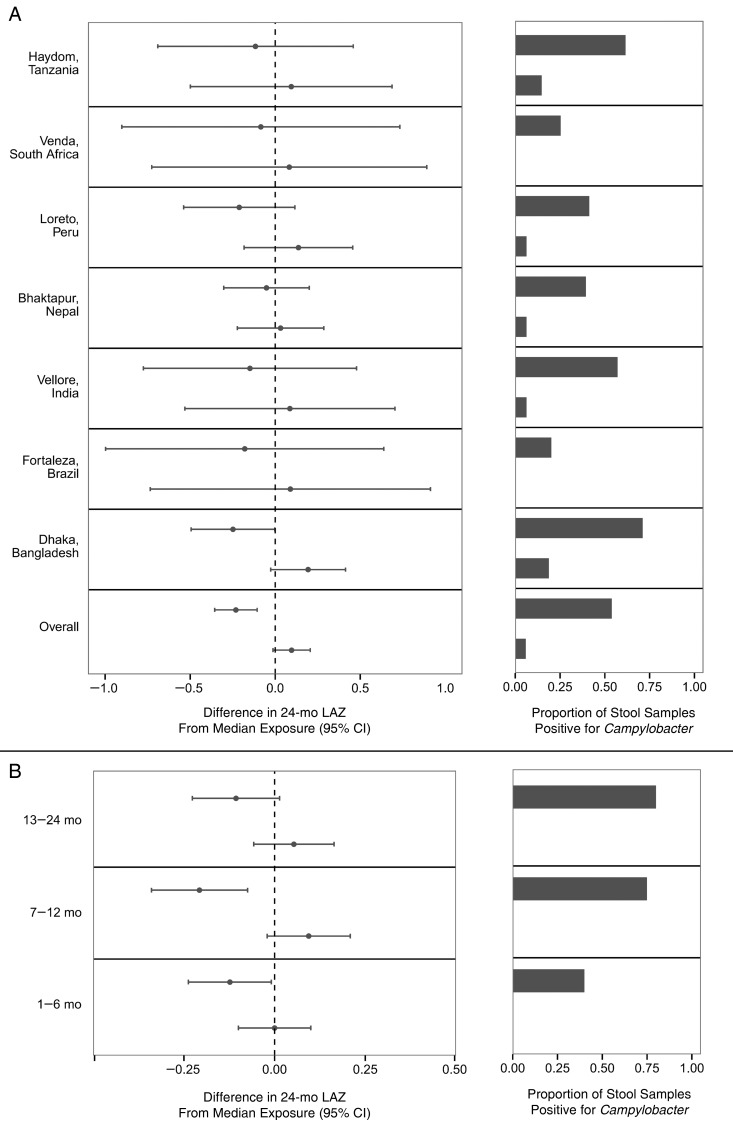
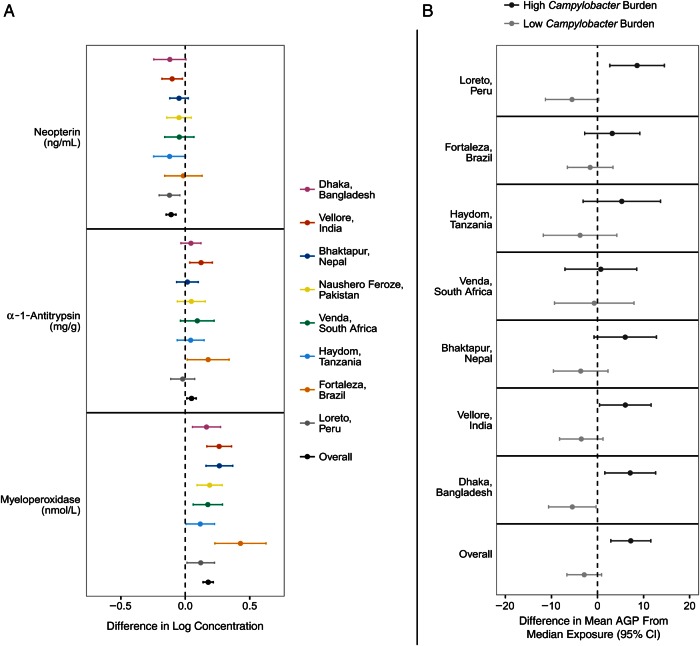
Results: A total of 1892 children had 7601 diarrheal and 26 267 nondiarrheal stool samples tested for Campylobacter We describe a high prevalence of infection, with most children (n = 1606; 84.9%) having a Campylobacter-positive stool sample by 1 year of age. Factors associated with a reduced risk of Campylobacter detection included exclusive breastfeeding (risk ratio, 0.57; 95% confidence interval, .47-.67), treatment of drinking water (0.76; 0.70-0.83), access to an improved latrine (0.89; 0.82-0.97), and recent macrolide antibiotic use (0.68; 0.63-0.74). A high Campylobacter burden was associated with a lower length-for-age Z score at 24 months (-1.82; 95% confidence interval, -1.94 to -1.70) compared with a low burden (-1.49; -1.60 to -1.38). This association was robust to confounders and consistent across sites. Campylobacter infection was also associated with increased intestinal permeability and intestinal and systemic inflammation.
Conclusions: Campylobacter was prevalent across diverse settings and associated with growth shortfalls. Promotion of exclusive breastfeeding, drinking water treatment, improved latrines, and targeted antibiotic treatment may reduce the burden of Campylobacter infection and improve growth in children in these settings.
Keywords: Campylobacter; children; growth; inflammation; risk factors.
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- Checkley W, Gilman RH, Epstein LD et al. . Asymptomatic and symptomatic cryptosporidiosis: their acute effect on weight gain in Peruvian children. Am J Epidemiol 1997; 145:156–63. - PubMed
-
- Lee G, Paredes Olortegui M, Penataro Yori P et al. . Effects of Shigella-, Campylobacter- and ETEC-associated diarrhea on childhood growth. Pediatric Infect Dis J 2014; 33:1004–9. - PubMed
-
- Black RE, Brown KH, Becker S. Effects of diarrhea associated with specific enteropathogens on the growth of children in rural Bangladesh. Pediatrics 1984; 73:799–805. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
