

Orthokeratinized Odontogenic Cyst with an Associated Keratocystic Odontogenic Tumor Component and Ghost Cell Keratinization and Calcifications in a Patient with Gardner Syndrome
- PMID: 27501963
- PMCID: PMC5429271
- DOI: 10.1007/s12105-016-0748-z
Orthokeratinized Odontogenic Cyst with an Associated Keratocystic Odontogenic Tumor Component and Ghost Cell Keratinization and Calcifications in a Patient with Gardner Syndrome
Abstract
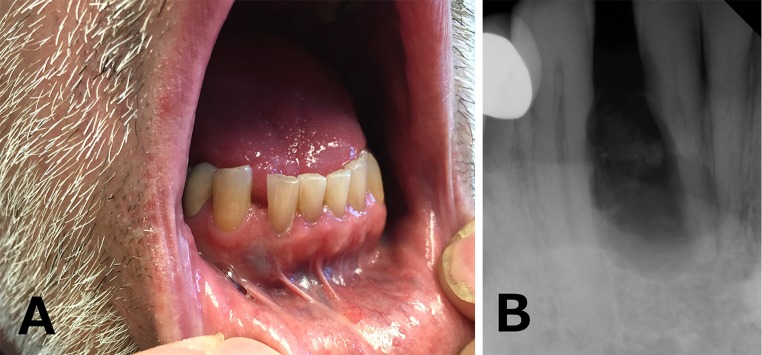
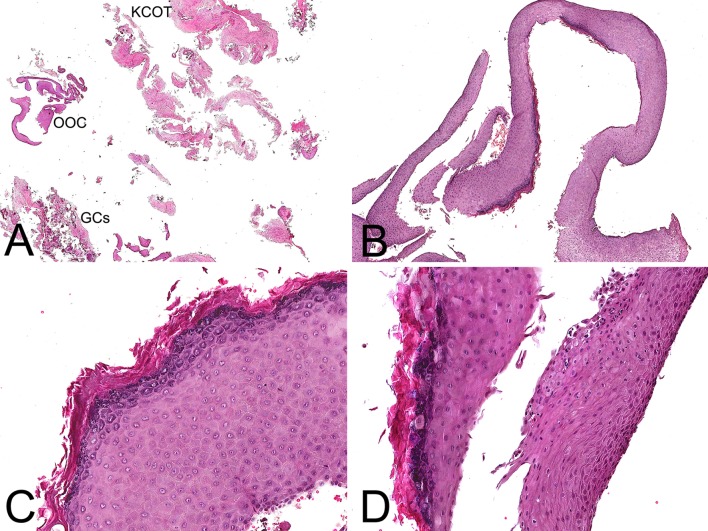
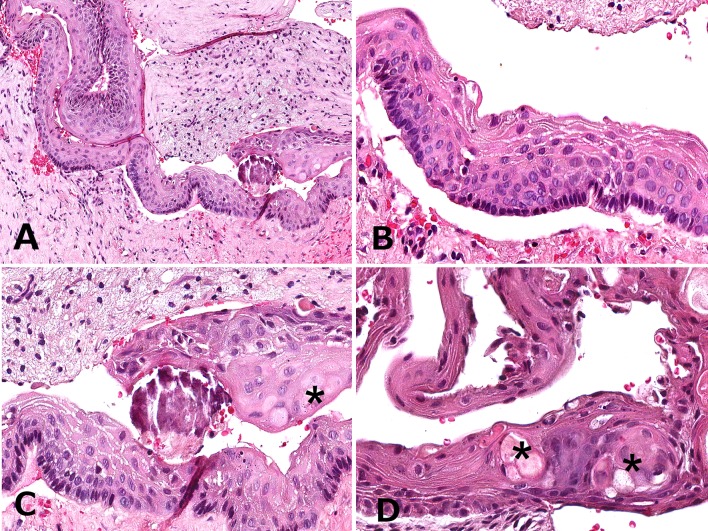
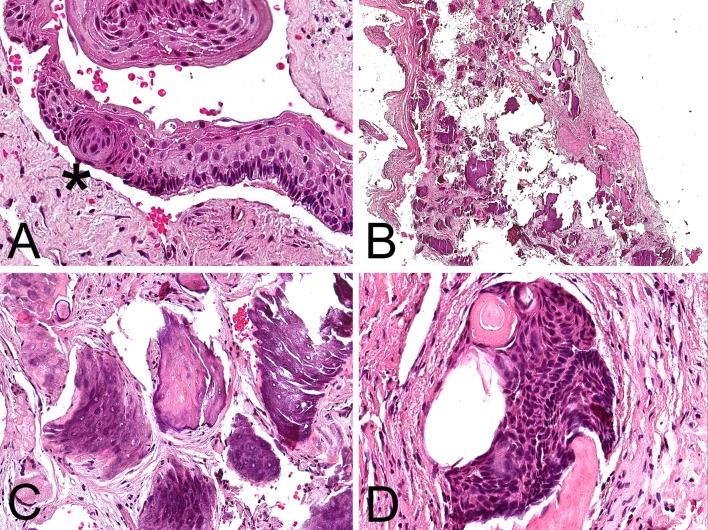
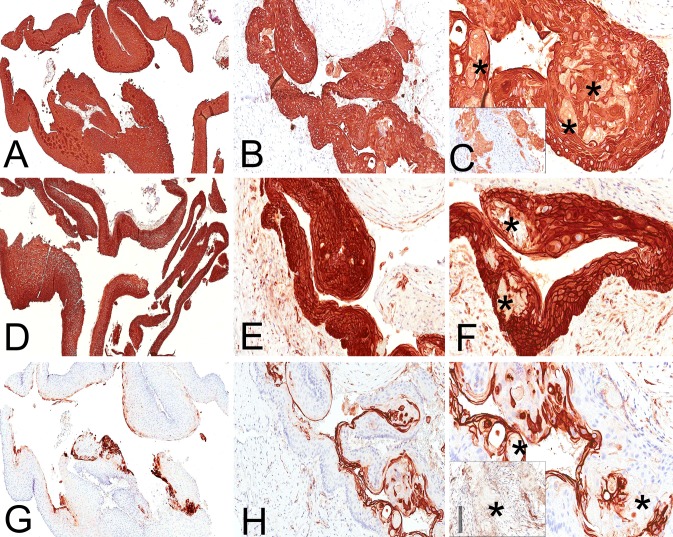
Gardner syndrome (GS) is caused by mutations in the APC and besides adenomatous colorectal polyps includes such manifestations as osteomas, epidermoid cysts (ECs) and occasionally multiple pilomatricomas. More than 50 % of ECs in patients with GS exhibit pilomatricoma-like ghost cell keratinization. The latter may be explained by the fact that the development of both GS and pilomatricoma is driven by activation of the Wnt/β-catenin signaling pathway. A 62-year-old, Caucasian male with history of GS presented with a unilocular, mixed radiopaque/radiolucent mandibular lesion causing divergence and external root resorption of involved teeth. Histopathologically, the lesion was composed of two cystic components, an orthokeratinized odontogenic cyst (OOC) and a smaller one with characteristics of keratocystic odontogenic tumor (KCOT) featuring, focally, ghost cells and an epithelial morule-like structure. Dystrophic calcifications essentially similar to those seen in pilomatricomas were observed in the fibrous connective tissue wall. The KCOT and OOC epithelia revealed strong and diffuse cytokeratin (AE1/AE3) and β-catenin immunoreactivity. CD10 positive immunostaining was seen in the keratin and superficial spinous cell layers in both OOC and KCOT. The intraepithelial and mural ghost cells showed a cytokeratin (+), β-catenin and CD10 (-) immunophenotype. The diagnosis of OOC with ghost cell calcifications in association with KCOT was rendered. The patient was lost to follow-up. Although a coincidental co-existence cannot be excluded, ghost cell calcifications mimicking pilomatricoma-like changes in an unusual odontogenic cyst combining OOC and KCOT features as seen in this patient with GS may be explained by the common molecular mechanisms underlying the pathogenesis of cutaneous pilomatricomas and GS.
Keywords: Gardner syndrome; Ghost cells; Keratocystic odontogenic tumor; Orthokeratinized odontogenic cyst; Pilomatricoma; β-catenin.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Ortho Keratinized Odontogenic Cyst with Dentinoid Formation.J Coll Physicians Surg Pak. 2017 Sep;27(9):S110-S111. J Coll Physicians Surg Pak. 2017. PMID: 28969743
-
Ghost cells in pilomatrixoma, craniopharyngioma, and calcifying cystic odontogenic tumor: histological, immunohistochemical, and ultrastructural study.J Oral Pathol Med. 2015 Apr;44(4):284-90. doi: 10.1111/jop.12234. Epub 2014 Jul 22. J Oral Pathol Med. 2015. PMID: 25047924
-
Calcifying Odontogenic Cyst Demonstrates Recurrent WNT Pathway Mutations and So-Called Adenoid Ameloblastoma-Like Histology: Evidence Supporting Its Classification as a Neoplasm.Mod Pathol. 2024 Jun;37(6):100484. doi: 10.1016/j.modpat.2024.100484. Epub 2024 Apr 2. Mod Pathol. 2024. PMID: 38574817
-
Odontogenic cysts, odontogenic tumors, fibroosseous, and giant cell lesions of the jaws.Mod Pathol. 2002 Mar;15(3):331-41. doi: 10.1038/modpathol.3880527. Mod Pathol. 2002. PMID: 11904346 Review.
-
Ghost Cell Odontogenic Carcinoma with Sarcomatous Transformation : Report of a Rare Case with Review of Literature.Gulf J Oncolog. 2023 Jan;1(41):111-116. Gulf J Oncolog. 2023. PMID: 36804166 Review.
Cited by
-
Orthokeratinized odontogenic cyst (OOC): Clinicopathological and radiological features of a series of 10 cases.Diagn Pathol. 2019 Apr 4;14(1):28. doi: 10.1186/s13000-019-0801-9. Diagn Pathol. 2019. PMID: 30947718 Free PMC article.
-
Calcifying Odontogenic Cyst Showing a Varied Epithelial Lining: An Additional Case with Implications for the Divergent Differentiation Capacity of the Cyst Epithelium.Head Neck Pathol. 2019 Jun;13(2):251-254. doi: 10.1007/s12105-018-0899-1. Epub 2018 Mar 28. Head Neck Pathol. 2019. PMID: 29594916 Free PMC article. No abstract available.
-
Ghost Cell Odontogenic Carcinoma of the Anterior Maxilla with ARID1A Mutation: A Case Report and Literature Review.Head Neck Pathol. 2025 Apr 25;19(1):46. doi: 10.1007/s12105-025-01785-z. Head Neck Pathol. 2025. PMID: 40279034 Review.
-
Osteoma of the Jaw as First Clinical Sign of Gardner's Syndrome: The Experience of Two Italian Centers and Review.J Clin Med. 2023 Feb 14;12(4):1496. doi: 10.3390/jcm12041496. J Clin Med. 2023. PMID: 36836031 Free PMC article.
-
Incidental finding of orthokeratinized odontogenic cyst with unusual features.J Oral Maxillofac Pathol. 2022 Jan-Mar;26(1):130. doi: 10.4103/jomfp.jomfp_133_21. Epub 2022 Mar 31. J Oral Maxillofac Pathol. 2022. PMID: 35571311 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
