

Cell-permeable succinate prodrugs bypass mitochondrial complex I deficiency
- PMID: 27502960
- PMCID: PMC4980488
- DOI: 10.1038/ncomms12317
Cell-permeable succinate prodrugs bypass mitochondrial complex I deficiency
Abstract
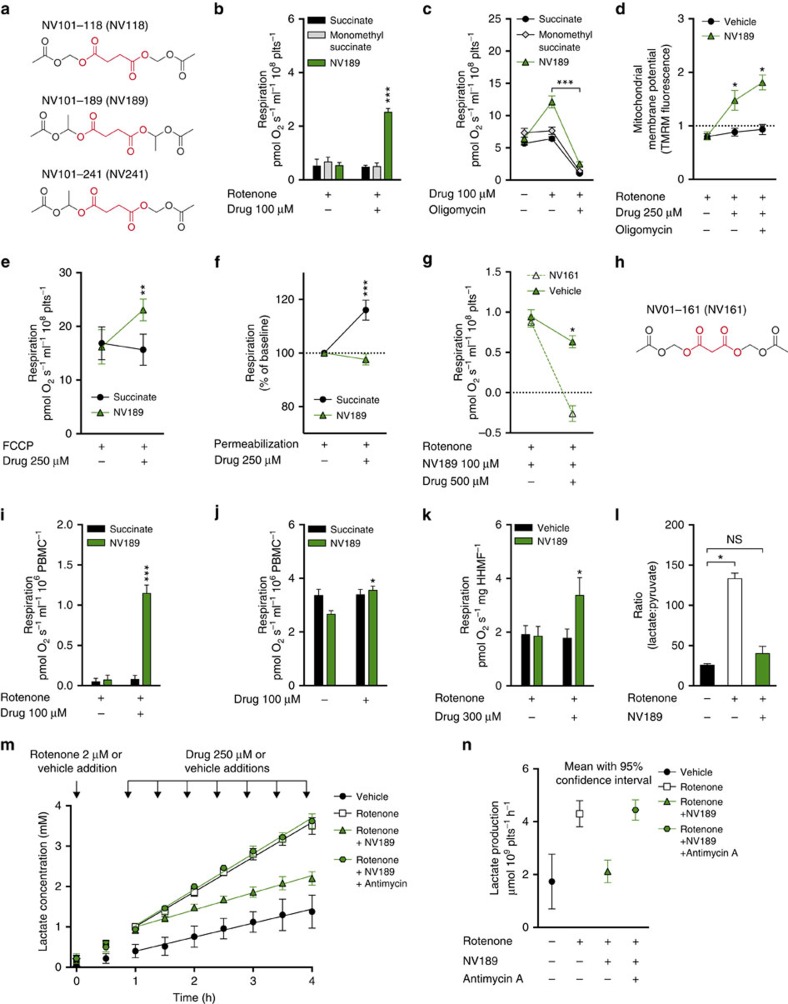
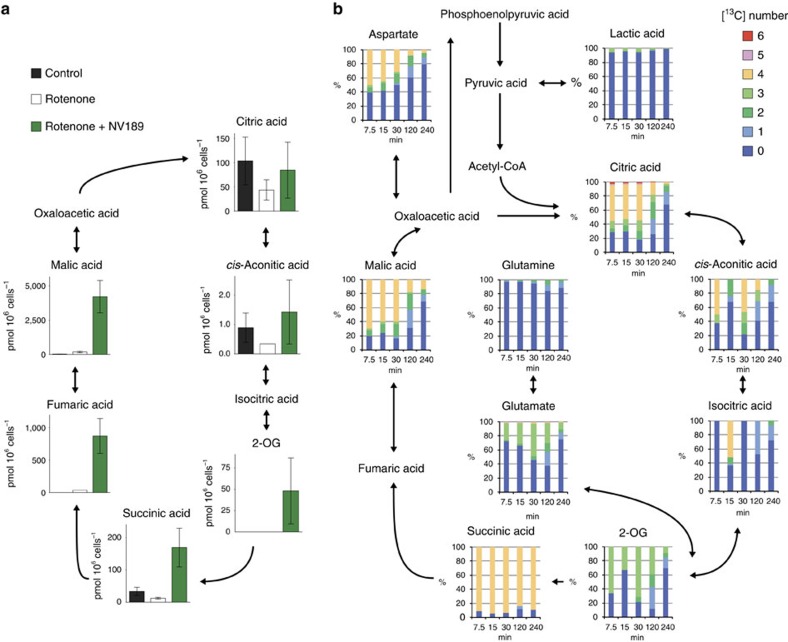
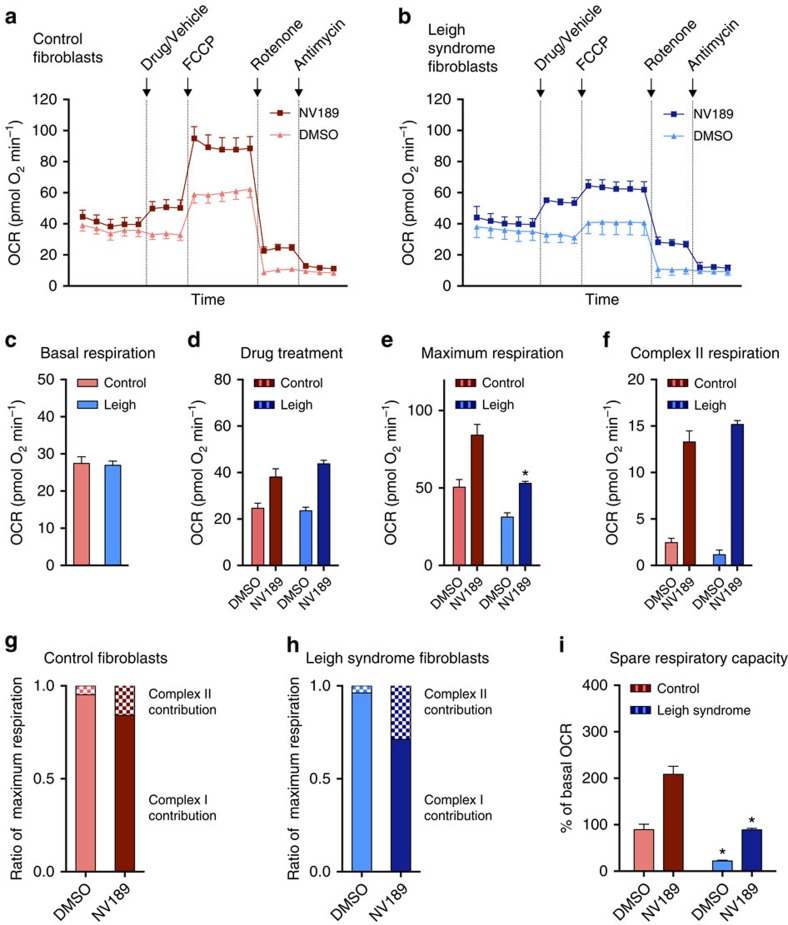
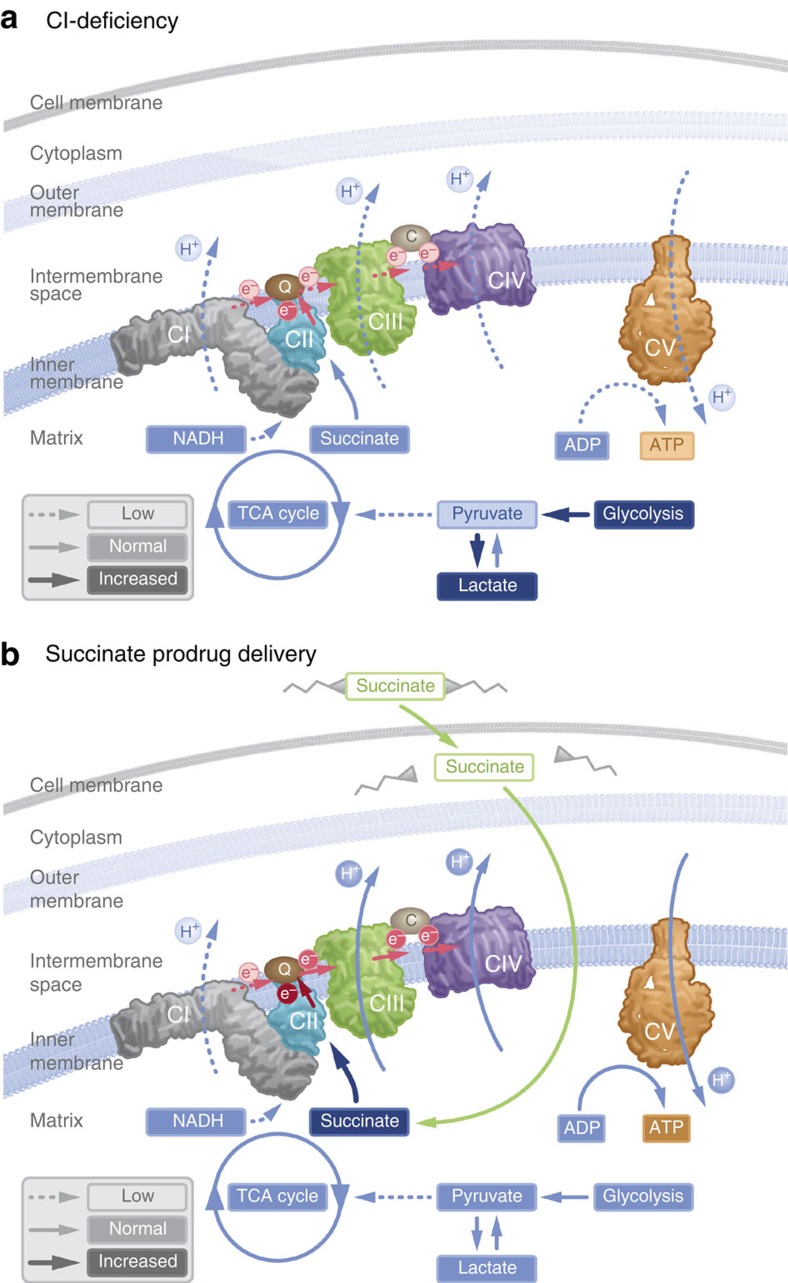
Mitochondrial complex I (CI) deficiency is the most prevalent defect in the respiratory chain in paediatric mitochondrial disease. This heterogeneous group of diseases includes serious or fatal neurological presentations such as Leigh syndrome and there are very limited evidence-based treatment options available. Here we describe that cell membrane-permeable prodrugs of the complex II substrate succinate increase ATP-linked mitochondrial respiration in CI-deficient human blood cells, fibroblasts and heart fibres. Lactate accumulation in platelets due to rotenone-induced CI inhibition is reversed and rotenone-induced increase in lactate:pyruvate ratio in white blood cells is alleviated. Metabolomic analyses demonstrate delivery and metabolism of [(13)C]succinate. In Leigh syndrome patient fibroblasts, with a recessive NDUFS2 mutation, respiration and spare respiratory capacity are increased by prodrug administration. We conclude that prodrug-delivered succinate bypasses CI and supports electron transport, membrane potential and ATP production. This strategy offers a potential future therapy for metabolic decompensation due to mitochondrial CI dysfunction.
Conflict of interest statement
This study is partly funded by NeuroVive Pharmaceutical AB and Selcia Ltd, companies active in the field of mitochondrial medicine. J.K.E., S.M., E.E., M.J.H., M.K., S.P., F.S., S.J.M. and E.Å.F. have or have had salary from and/or equity interest in NeuroVive Pharmaceutical. H.F., R.F. and C.C. have or have had salary from and/or equity interest in Selcia Ltd/Mitopharm Ltd.
Figures
References
-
- Distelmaier F. et al. Mitochondrial complex I deficiency: from organelle dysfunction to clinical disease. Brain 132, 833–842 (2009). - PubMed
-
- Lightowlers R. N., Taylor R. W. & Turnbull D. M. Mutations causing mitochondrial disease: What is new and what challenges remain? Science 349, 1494–1499 (2015). - PubMed
-
- Fliri H. et al. Protected succinates for enhancing mitochondrial ATP-production. Patent WO2014053857 A1 (2014).
-
- MacDonald M. J., Fahien L. A., Mertz R. J. & Rana R. S. Effect of esters of succinic acid and other citric acid cycle intermediates on insulin release and inositol phosphate formation by pancreatic islets. Arch. Biochem. Biophys. 269, 400–406 (1989). - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
