

Prospective evaluation of SeptiFast Multiplex PCR in children with systemic inflammatory response syndrome under antibiotic treatment
- PMID: 27503068
- PMCID: PMC4977629
- DOI: 10.1186/s12879-016-1722-9
Prospective evaluation of SeptiFast Multiplex PCR in children with systemic inflammatory response syndrome under antibiotic treatment
Abstract
Background: Antimicrobially pre-treated children with systemic inflammation often pose a diagnostic challenge to the physician. We aimed to evaluate the additional use of SeptiFast multiplex polymerase chain reaction (PCR) to identify causative pathogens in children with suspected systemic bacterial or fungal infection.
Methods: Prospective observational study in 39 children with systemic inflammatory response syndrome (SIRS) under empiric antibiotic treatment. Primary outcome was the rate of positive blood cultures (BC), compared to the rate of positive SeptiFast (SF) results.
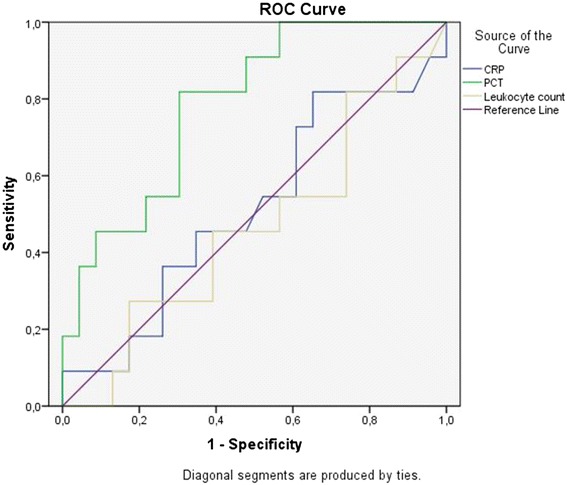
Results: In total, 14 SF-samples yielded positive results, compared to 4 positive BC (p < 0.05). All blood cultures and 13 of 14 positive SF-tests were considered infection. Median time for positive BC was 2 days, and time to definite result was 6 days, compared to 12 h for SF. Antimicrobial therapy was adapted in 7 of the 14 patients with positive SeptiFast, and in 3 of the 4 patients with positive BC. Best predictive power for positive SF shown by receiver-operating characteristic was demonstrated for procalcitonin PCT (Area under the curve AUC: 0.79), compared to C-reactive protein CRP (AUC: 0.51) and leukocyte count (AUC: 0.46). A procalcitonin threshold of 0.89 ng/ml yielded a sensitivity of 0.82 and a specifity of 0.7. Children with a positive SeptiFast result on day 0 had a significantly higher risk to require treatment on the Pediatric Intensive Care Unit or to be deceased on day 30 (Odds-Ratio 8.62 (CI 1.44-51.72).
Conclusions: The additional testing with SeptiFast in antimicrobially pre-treated children with systemic inflammation enhances the rate of pathogen detection. The influence of multiplex PCR on clinically relevant outcome parameters has to be further evaluated. (
Trial registration: DRKS00004694).
Keywords: Antimicrobial treatment; Blood culture; Children; SeptiFast; Systemic Inflammatory Response Syndrome (SIRS).
Figures
References
-
- Garnacho-Montero J, Garcia-Garmendia JL, Barrero-Almodovar A, Jimenez-Jimenez FJ, Perez-Paredes C, Ortiz-Leyba C. Impact of adequate empirical antibiotic therapy on the outcome of patients admitted to the intensive care unit with sepsis. Crit Care Med. 2003;31(12):2742–2751. doi: 10.1097/01.CCM.0000098031.24329.10. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
