

A combination of TERT promoter mutation and MGMT methylation status predicts clinically relevant subgroups of newly diagnosed glioblastomas
- PMID: 27503138
- PMCID: PMC4977715
- DOI: 10.1186/s40478-016-0351-2
A combination of TERT promoter mutation and MGMT methylation status predicts clinically relevant subgroups of newly diagnosed glioblastomas
Abstract
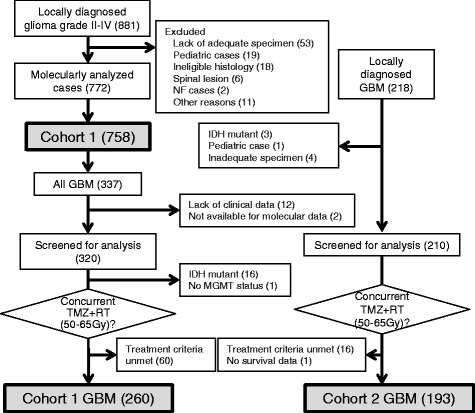
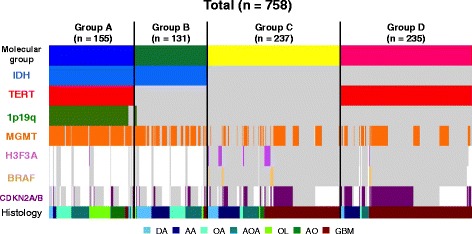
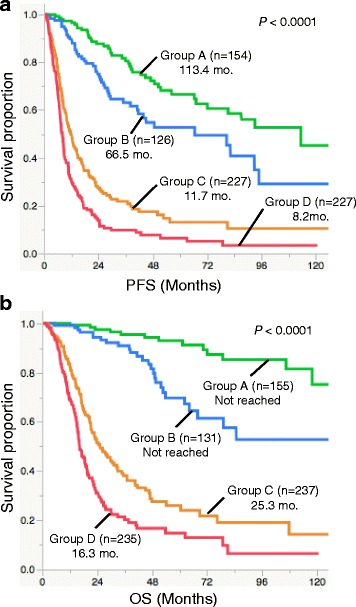
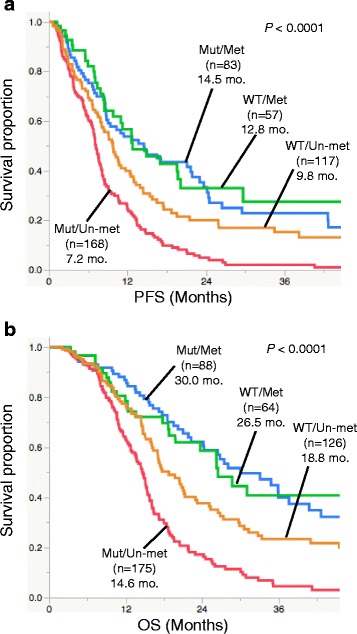
The prognostic impact of TERT mutations has been controversial in IDH-wild tumors, particularly in glioblastomas (GBM). The controversy may be attributable to presence of potential confounding factors such as MGMT methylation status or patients' treatment. This study aimed to evaluate the impact of TERT status on patient outcome in association with various factors in a large series of adult diffuse gliomas. We analyzed a total of 951 adult diffuse gliomas from two cohorts (Cohort 1, n = 758; Cohort 2, n = 193) for IDH1/2, 1p/19q, and TERT promoter status. The combined IDH/TERT classification divided Cohort 1 into four molecular groups with distinct outcomes. The overall survival (OS) was the shortest in IDH wild-type/TERT mutated groups, which mostly consisted of GBMs (P < 0.0001). To investigate the association between TERT mutations and MGMT methylation on survival of patients with GBM, samples from a combined cohort of 453 IDH-wild-type GBM cases treated with radiation and temozolomide were analyzed. A multivariate Cox regression model revealed that the interaction between TERT and MGMT was significant for OS (P = 0.0064). Compared with TERT mutant-MGMT unmethylated GBMs, the hazard ratio (HR) for OS incorporating the interaction was the lowest in the TERT mutant-MGMT methylated GBM (HR, 0.266), followed by the TERT wild-type-MGMT methylated (HR, 0.317) and the TERT wild-type-MGMT unmethylated GBMs (HR, 0.542). Thus, patients with TERT mutant-MGMT unmethylated GBM have the poorest prognosis. Our findings suggest that a combination of IDH, TERT, and MGMT refines the classification of grade II-IV diffuse gliomas.
Keywords: 1p19q; Glioblastoma; Glioma; IDH1/2; Molecular classification; Prognostic factor; TERT; Temozolomide.
Figures
References
-
- Arita H, Narita Y, Fukushima S, Tateishi K, Matsushita Y, Yoshida A, Miyakita Y, Ohno M, Collins VP, Kawahara N, Shibui S, Ichimura K. Upregulating mutations in the TERT promoter commonly occur in adult malignant gliomas and are strongly associated with total 1p19q loss. Acta Neuropathol. 2013;126:267–76. doi: 10.1007/s00401-013-1141-6. - DOI - PubMed
-
- Bell RJ, Rube HT, Kreig A, Mancini A, Fouse SD, Nagarajan RP, Choi S, Hong C, He D, Pekmezci M, Wiencke JK, Wrensch MR, Chang SM, Walsh KM, Myong S, Song JS, Costello JF. Cancer. The transcription factor GABP selectively binds and activates the mutant TERT promoter in cancer. Science. 2015;348:1036–9. doi: 10.1126/science.aab0015. - DOI - PMC - PubMed
-
- Bettegowda C, Agrawal N, Jiao Y, Sausen M, Wood LD, Hruban RH, Rodriguez FJ, Cahill DP, McLendon R, Riggins G, Velculescu VE, Oba-Shinjo SM, Marie SK, Vogelstein B, Bigner D, Yan H, Papadopoulos N, Kinzler KW. Mutations in CIC and FUBP1 contribute to human oligodendroglioma. Science. 2011;333:1453–5. doi: 10.1126/science.1210557. - DOI - PMC - PubMed
-
- Ceccarelli M, Barthel FP, Malta TM, Sabedot TS, Salama SR, Murray BA, Morozova O, Newton Y, Radenbaugh A, Pagnotta SM, Anjum S, Wang J, Manyam G, Zoppoli P, Ling S, Rao AA, Grifford M, Cherniack AD, Zhang H, Poisson L, Carlotti CG, Jr, Tirapelli DP, Rao A, Mikkelsen T, Lau CC, Yung WK, Rabadan R, Huse J, Brat DJ, Lehman NL, Barnholtz-Sloan JS, Zheng S, Hess K, Rao G, Meyerson M, Beroukhim R, Cooper L, Akbani R, Wrensch M, Haussler D, Aldape KD, Laird PW, Gutmann DH, Network TR, Noushmehr H, Iavarone A, Verhaak RG. Molecular Profiling Reveals Biologically Discrete Subsets and Pathways of Progression in Diffuse Glioma. Cell. 2016;164:550–63. doi: 10.1016/j.cell.2015.12.028. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
