

Ultrasound-guided therapeutic modulation of hepatocellular carcinoma using complementary microRNAs
- PMID: 27503707
- PMCID: PMC5185600
- DOI: 10.1016/j.jconrel.2016.08.005
Ultrasound-guided therapeutic modulation of hepatocellular carcinoma using complementary microRNAs
Abstract
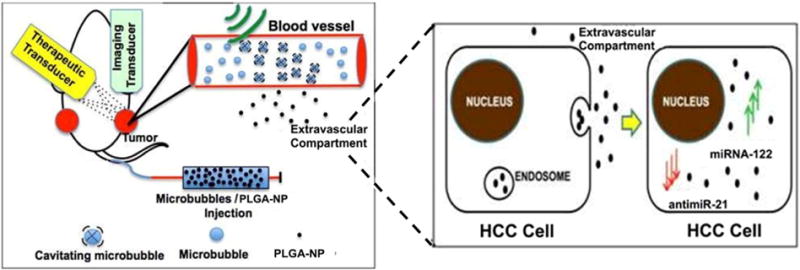
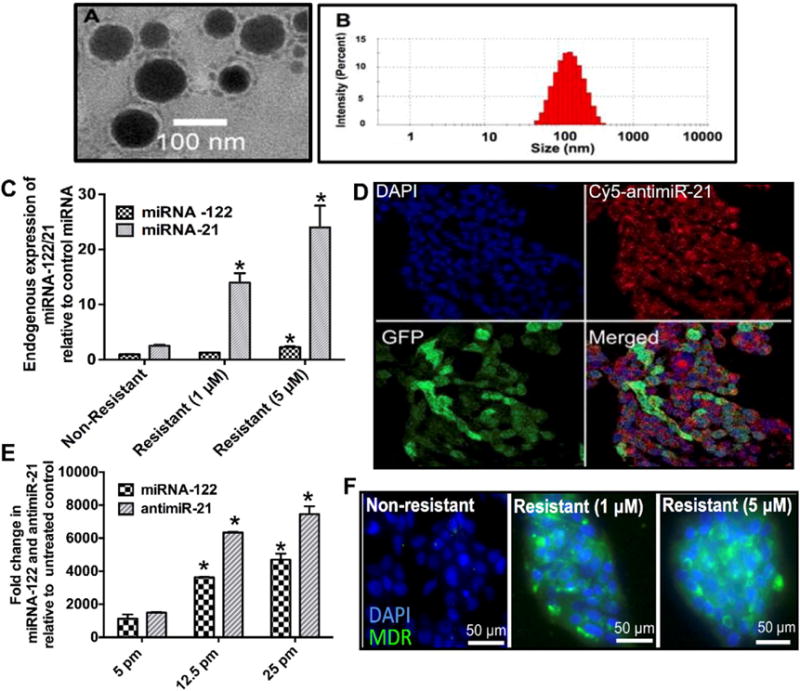
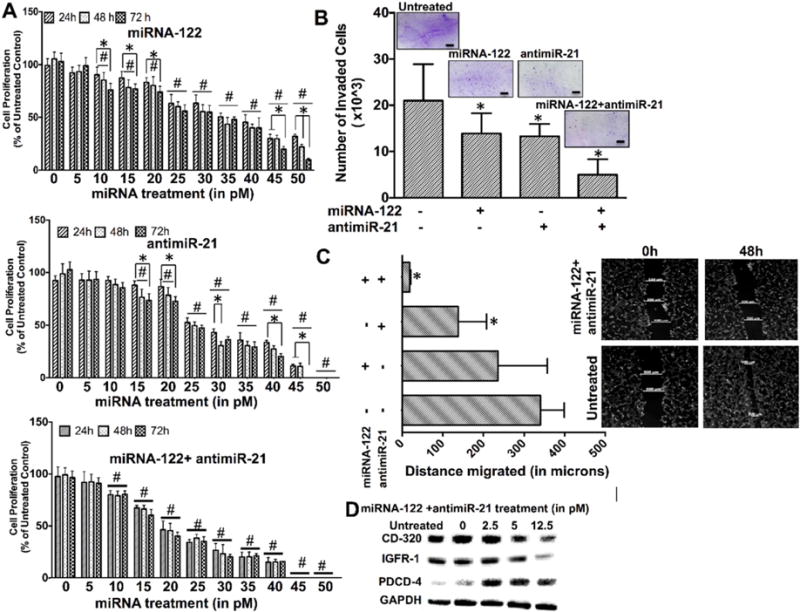
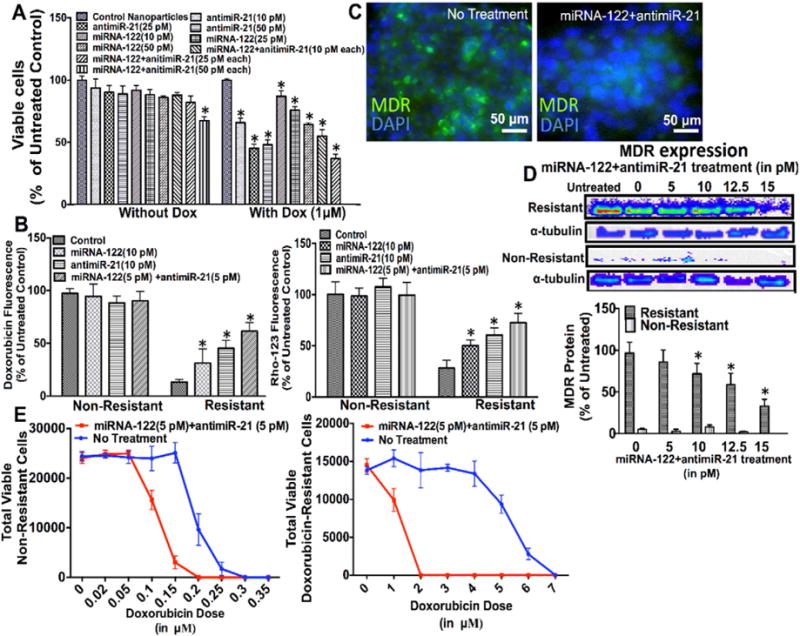
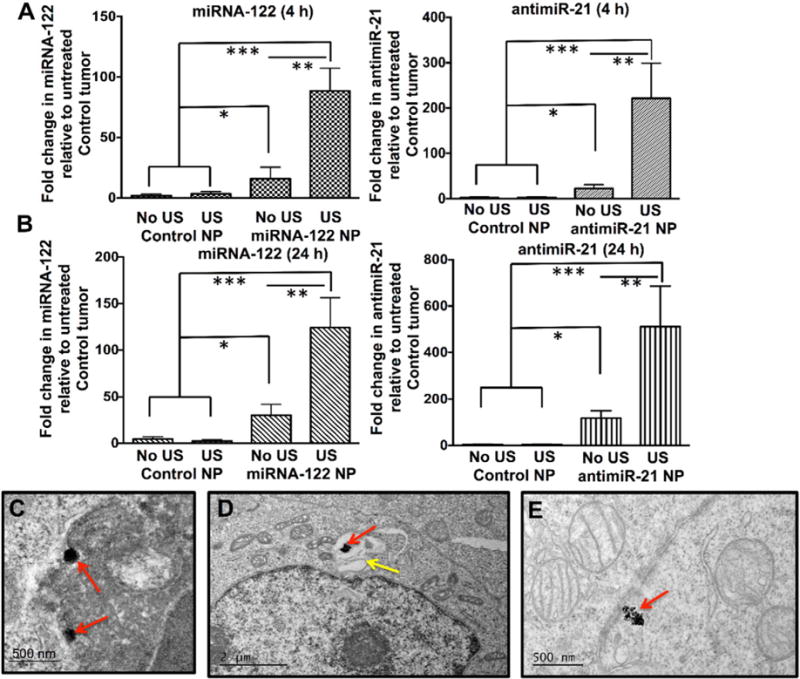
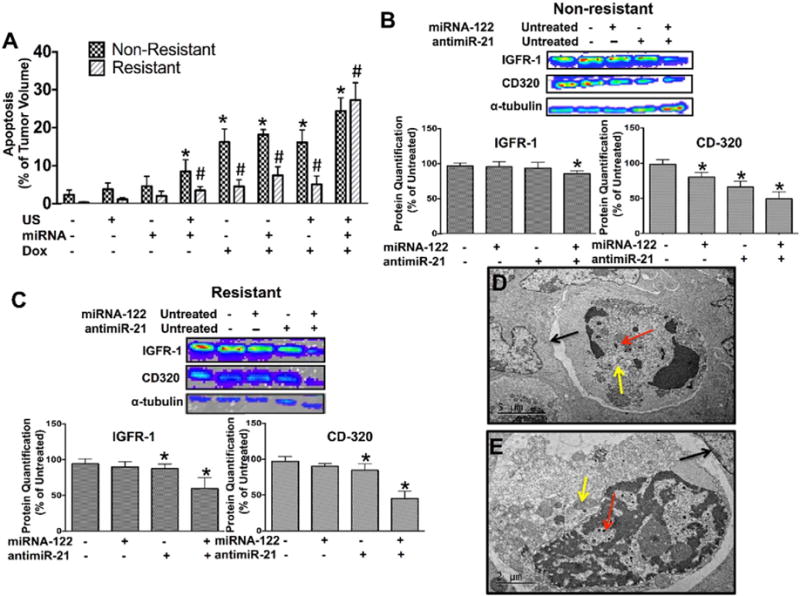
Treatment options for patients with hepatocellular carcinoma (HCC) are limited, in particular in advanced and drug resistant HCC. MicroRNAs (miRNA) are non-coding small RNAs that are emerging as novel drugs for the treatment of cancer. The aim of this study was to assess treatment effects of two complementary miRNAs (sense miRNA-122, and antisense antimiR-21) encapsulated in biodegradable poly (lactic-co-glycolic acid) nanoparticles (PLGA-NP), administered by an ultrasound-guided and microbubble-enhanced delivery approach in doxorubicin-resistant and non-resistant human HCC xenografts. Proliferation and invasiveness of human HCC cells after miRNA-122/antimiR-21 and doxorubicin treatment were assessed in vitro. Confocal microscopy and qRT-PCR were used to visualize and quantitate successful intracellular miRNA-loaded PLGA-NP delivery. Up and down-regulation of miRNA downstream targets and multidrug resistance proteins and extent of apoptosis were assessed in vivo in treated human HCC xenografts in mice. Compared to single miRNA therapy, combination therapy with the two complementary miRNAs resulted in significantly (P<0.05) stronger decrease in cell proliferation, invasion, and migration of HCC cells as well as higher resensitization to doxorubicin. Ultrasound-guided delivery significantly increased in vivo miRNA-loaded PLGA-NP delivery in human HCC xenografts compared to control conditions by 5-9 fold (P<0.001). miRNA-loaded PLGA-NP were internalized in HCC cells and anti-apoptotic proteins were down regulated with apoptosis in ~27% of the tumor volume of doxorubicin-resistant human HCC after a single treatment with complementary miRNAs and doxorubicin. Thus, ultrasound-guided delivery of complementary miRNAs is highly efficient in the treatment of doxorubicin- resistant and non-resistant HCC. Further development of this new treatment approach could aid in better treatment of patients with HCC.
Keywords: Cancer therapy; Complementary miRNA; Drug resistance; Hepatocellular carcinoma; Ultrasound.
Copyright © 2016 Elsevier B.V. All rights reserved.
Conflict of interest statement
of potential conflicts of interest There is no actual or potential conflicts of interest with regard to this paper.
Figures
References
-
- Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet. 2012;379:1245–1255. - PubMed
-
- E.A.f.S.o. Liver. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. Eur J Cancer. 2012;48:599. - PubMed
-
- Lencioni R, Cioni D, Crocetti L, Bartolozzi C. Percutaneous ablation of hepatocellular carcinoma: state-of-the-art. Liver Transpl. 2004;10:S91–S97. - PubMed
-
- Llovet JM, Fuster J, Bruix J. Intention-to-treat analysis of surgical treatment for early hepatocellular carcinoma: resection versus transplantation. Hepatology. 1999;30:1434–1440. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
