

International consensus on the diagnosis and management of pediatric patients with hereditary angioedema with C1 inhibitor deficiency
- PMID: 27503784
- PMCID: PMC5248622
- DOI: 10.1111/all.13001
International consensus on the diagnosis and management of pediatric patients with hereditary angioedema with C1 inhibitor deficiency
Abstract
Background: The consensus documents published to date on hereditary angioedema with C1 inhibitor deficiency (C1-INH-HAE) have focused on adult patients. Many of the previous recommendations have not been adapted to pediatric patients. We intended to produce consensus recommendations for the diagnosis and management of pediatric patients with C1-INH-HAE.
Methods: During an expert panel meeting that took place during the 9th C1 Inhibitor Deficiency Workshop in Budapest, 2015 (www.haenet.hu), pediatric data were presented and discussed and a consensus was developed by voting.
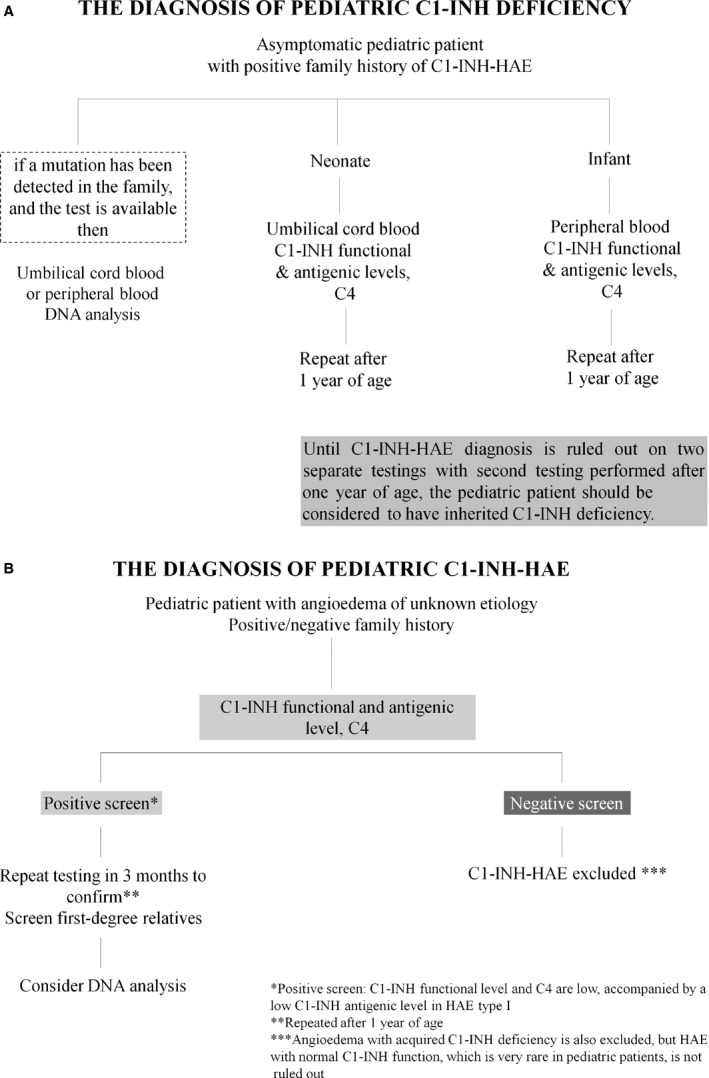
Results: The symptoms of C1-INH-HAE often present in childhood. Differential diagnosis can be difficult as abdominal pain is common in pediatric C1-INH-HAE, but also commonly occurs in the general pediatric population. The early onset of symptoms may predict a more severe subsequent course of the disease. Before the age of 1 year, C1-INH levels may be lower than in adults; therefore, it is advisable to confirm the diagnosis after the age of one year. All neonates/infants with an affected C1-INH-HAE family member should be screened for C1-INH deficiency. Pediatric patients should always carry a C1-INH-HAE information card and medicine for emergency use. The regulatory approval status of the drugs for prophylaxis and for acute treatment is different in each country. Plasma-derived C1-INH, recombinant C1-INH, and ecallantide are the only agents licensed for the acute treatment of pediatric patients. Clinical trials are underway with additional drugs. It is recommended to follow up patients in an HAE comprehensive care center.
Conclusions: The pediatric-focused international consensus for the diagnosis and management of C1-INH-HAE patients was created.
Keywords: C1 inhibitor deficiency; diagnosis; hereditary angioedema; management; pediatric.
© 2016 The Authors. Allergy Published by John Wiley & Sons Ltd.
Figures
References
-
- Agostoni A, Cicardi M. Hereditary and acquired C1‐inhibitor deficiency: biological and clinical characteristics in 235 patients. Medicine (Baltimore) 1992;71:206–215. - PubMed
-
- Bork K, Meng G, Staubach P, Hardt J. Hereditary angioedema: new findings concerning symptoms, affected organs, and course. Am J Med 2006;119:267–274. - PubMed
-
- Martinez‐Saguer I, Farkas H. Erythema marginatum as an early symptom of hereditary angioedema: case report of 2 newborns. Pediatrics 2016;137:e20152411. - PubMed
-
- Bennett G, Craig T. Hereditary angioedema with a focus on the child. Allergy Asthma Proc 2015;36:70–73. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
