

Prognostic Value of the Change in Heart Rate From the Supine to the Upright Position in Patients With Chronic Heart Failure
- PMID: 27503849
- PMCID: PMC5015278
- DOI: 10.1161/JAHA.116.003524
Prognostic Value of the Change in Heart Rate From the Supine to the Upright Position in Patients With Chronic Heart Failure
Abstract
Background: The prognostic value of the change in heart rate from the supine to upright position (∆HR) in patients with chronic heart failure (HF) is unknown.
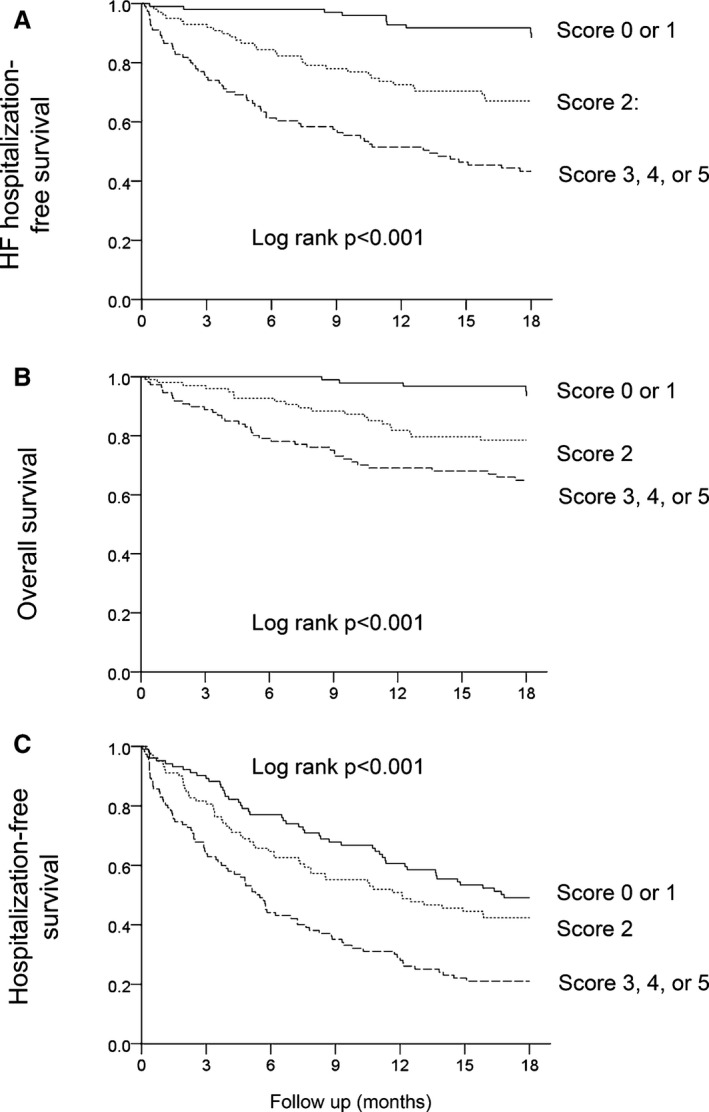
Methods and results: ∆HR was measured in patients enrolled in the Trial of Intensified Medical Therapy in Elderly Patients with Congestive Heart Failure (TIME-CHF) who were in sinus rhythm and had no pacemaker throughout the trial (n=321). The impact of ∆HR on 18-month outcome (HF hospitalization-free survival) was assessed. In addition, the prognostic effect of changes in ∆HR between baseline and month 6 on outcomes in the following 12 months was determined. A lower ∆HR was associated with a higher risk of death or HF hospitalization (hazard ratio 1.79 [95% confidence interval {95% CI} 1.19-2.75] if ∆HR ≤3 beats/min [bpm], P=0.004). In the multivariate analysis, lower ∆HR remained an independent predictor of death or HF hospitalization (hazard ratio 1.75 [95% CI, 1.18-2.61] if ∆HR ≤3 bpm, P=0.004) along with ischemic HF etiology, lower estimated glomerular filtration rate, presence and extent of rales, and no baseline β-blocker use. In patients without event during the first 6 months, the change in ∆HR from baseline to month 6 predicted death or HF hospitalization during the following 12 months (hazard ratio=2.13 [95% CI 1.12-5.00] if rise in ∆HR <2 bpm; P=0.027).
Conclusions: ∆HR as a simple bedside test is an independent prognostic predictor in patients with chronic HF. ∆HR is modifiable, and changes in ∆HR also provide prognostic information, which raises the possibility that ∆HR may help to guide treatment.
Clinical trial registration information: URL: www.isrctn.org. Unique identifier: ISRCTN43596477.
Keywords: TIME‐CHF; autonomic nervous system; heart failure; heart rate/heart rate variability; prognosis.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures


References
-
- Kaye DM, Lefkovits J, Jennings GL, Bergin P, Broughton A, Esler MD. Adverse consequences of high sympathetic nervous activity in the failing human heart. J Am Coll Cardiol. 1995;26:1257–1263. - PubMed
-
- Arena R, Guazzi M, Myers J, Peberdy MA. Prognostic value of heart rate recovery in patients with heart failure. Am Heart J. 2006;151:851.e7 851.e13 - PubMed
-
- Mortara A, La Rovere MT, Signorini MG, Pantaleo P, Pinna G, Martinelli L, Ceconi C, Cerutti S, Tavazzi L. Can power spectral analysis of heart rate variability identify a high risk subgroup of congestive heart failure patients with excessive sympathetic activation? A pilot study before and after heart transplantation. Br Heart J. 1994;71:422–430. - PMC - PubMed
-
- Mortara A, La Rovere MT, Pinna GD, Prpa A, Maestri R, Febo O, Pozzoli M, Opasich C, Tavazzi L. Arterial baroreflex modulation of heart rate in chronic heart failure: clinical and hemodynamic correlates and prognostic implications. Circulation. 1997;96:3450–3458. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
