

Relevance of New Definitions to Incidence and Prognosis of Acute Kidney Injury in Hospitalized Patients with Cirrhosis: A Retrospective Population-Based Cohort Study
- PMID: 27504876
- PMCID: PMC4978466
- DOI: 10.1371/journal.pone.0160394
Relevance of New Definitions to Incidence and Prognosis of Acute Kidney Injury in Hospitalized Patients with Cirrhosis: A Retrospective Population-Based Cohort Study
Abstract
Background: The implementation of new serum creatinine (SCr)-based criteria for acute kidney injury (AKI) has brought to light several areas of uncertainty in patients with cirrhosis.
Study design: Population-based cohort study.
Setting & participants: Adults with cirrhosis hospitalized between 2002-2012.
Predictor: We aimed to address the prognostic implications of the new AKI criteria in cirrhosis.
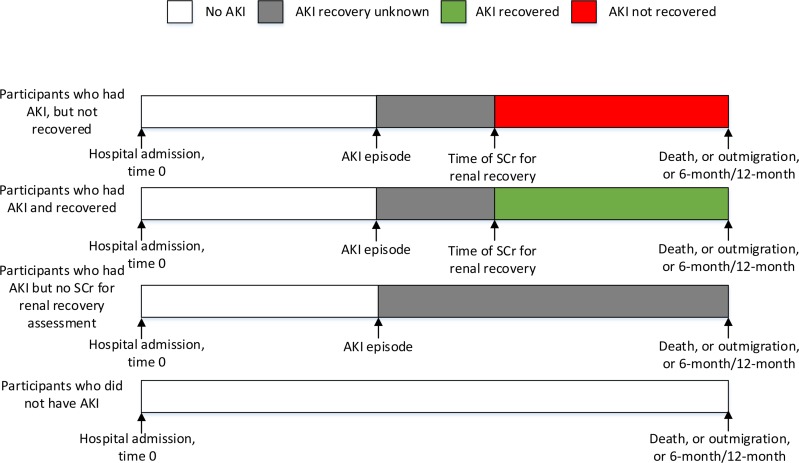
Outcomes: Baseline kidney function was defined from all outpatient SCr within 3 months before hospitalization. Cox proportional hazards models were fit to examine associations between AKI, renal recovery and all-cause mortality.
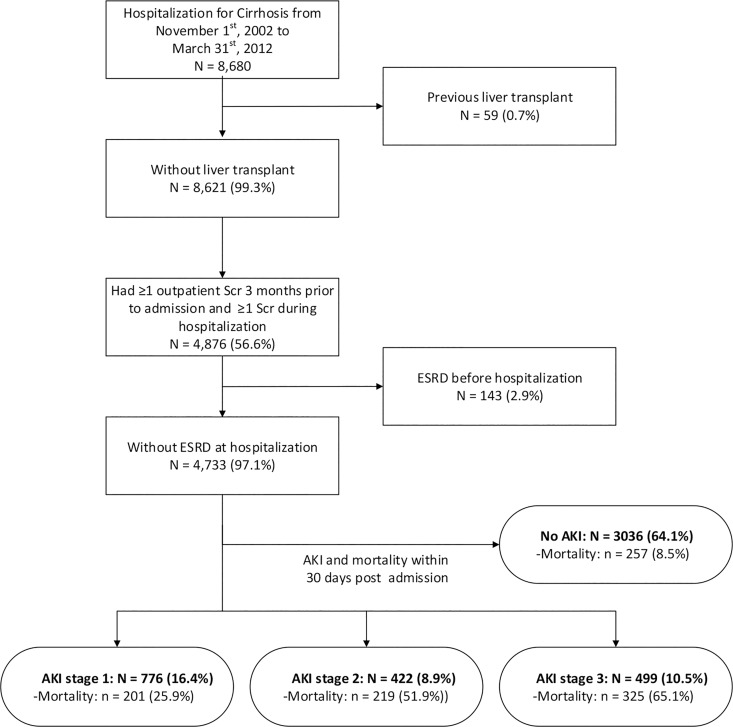
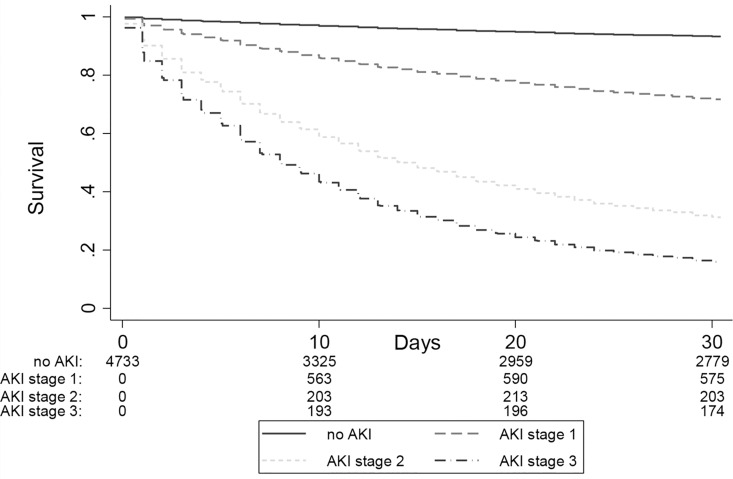
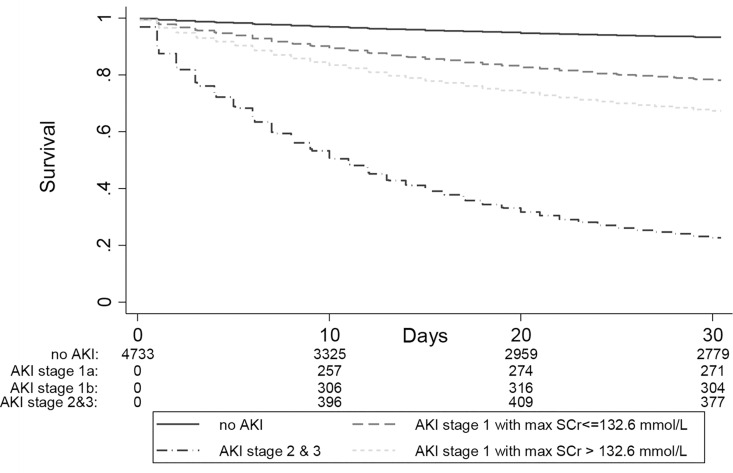
Results: 4,733 patients were studied. The 30-day mortality was higher for participants with AKI (43.9% vs 8.5%; p-value<0.001), and increased with AKI severity. The highest incidence of AKI occurred when the lowest SCr within the three months prior to admission was used to define baseline. The hazard ratio for mortality using the lowest SCr within 3 months and the closest pre-admission SCr (definition suggested by the recent consensus guideline) were similar, validating the use of the latter measure. As compared to patients without AKI, stage 1 AKI with maximum SCr ≤132 mmol/L remained associated with a 3.5-fold increased hazard of death at 30 days (95% CI 2.6 to 4.7).
Limitations: As an observational study, the results were vulnerable to residual confounding and ascertainment bias in the use of laboratory data to identify AKI. We did not have access to liver function or disease etiology variables and were unable to adjust for these in our analyses.
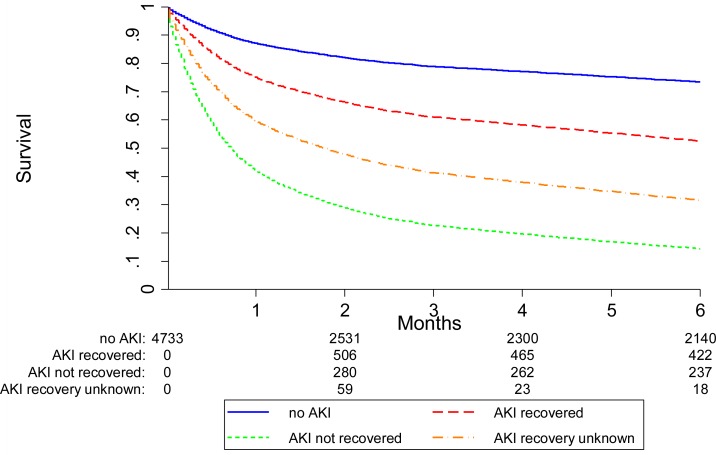
Conclusions: These results confirm the graded relationship between AKI severity, renal recovery, and mortality and further clarify previously discordant reports about the prognostic relevance of new AKI criteria in patients with cirrhosis.
Conflict of interest statement
Figures
References
-
- Wong F, O'Leary JG, Reddy KR, Patton H, Kamath PS, Fallon MB, et al. New consensus definition of acute kidney injury accurately predicts 30-day mortality in patients with cirrhosis and infection. Gastroenterology. 2013;145(6):1280–8 e1. Epub 2013/09/04. 10.1053/j.gastro.2013.08.051 . - DOI - PMC - PubMed
-
- Arroyo V, Gines P, Gerbes AL, Dudley FJ, Gentilini P, Laffi G, et al. Definition and diagnostic criteria of refractory ascites and hepatorenal syndrome in cirrhosis. Hepatology. 1996;23:164–76. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
