

Evaluation of a Urine Pooling Strategy for the Rapid and Cost-Efficient Prevalence Classification of Schistosomiasis
- PMID: 27504954
- PMCID: PMC4978437
- DOI: 10.1371/journal.pntd.0004894
Evaluation of a Urine Pooling Strategy for the Rapid and Cost-Efficient Prevalence Classification of Schistosomiasis
Abstract
Background: A key epidemiologic feature of schistosomiasis is its focal distribution, which has important implications for the spatial targeting of preventive chemotherapy programs. We evaluated the diagnostic accuracy of a urine pooling strategy using a point-of-care circulating cathodic antigen (POC-CCA) cassette test for detection of Schistosoma mansoni, and employed simulation modeling to test the classification accuracy and efficiency of this strategy in determining where preventive chemotherapy is needed in low-endemicity settings.
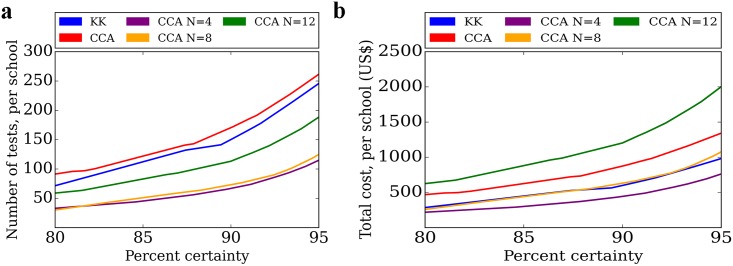
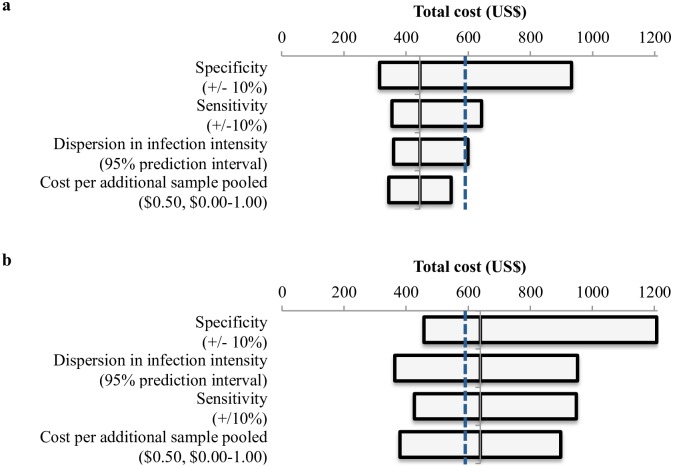
Methodology: We performed a cross-sectional study involving 114 children aged 6-15 years in six neighborhoods in Azaguié Ahoua, south Côte d'Ivoire to characterize the sensitivity and specificity of the POC-CCA cassette test with urine samples that were tested individually and in pools of 4, 8, and 12. We used a Bayesian latent class model to estimate test characteristics for individual POC-CCA and quadruplicate Kato-Katz thick smears on stool samples. We then developed a microsimulation model and used lot quality assurance sampling to test the performance, number of tests, and total cost per school for each pooled testing strategy to predict the binary need for school-based preventive chemotherapy using a 10% prevalence threshold for treatment.
Principal findings: The sensitivity of the urine pooling strategy for S. mansoni diagnosis using pool sizes of 4, 8, and 12 was 85.9%, 79.5%, and 65.4%, respectively, when POC-CCA trace results were considered positive, and 61.5%, 47.4%, and 30.8% when POC-CCA trace results were considered negative. The modeled specificity ranged from 94.0-97.7% for the urine pooling strategies (when POC-CCA trace results were considered negative). The urine pooling strategy, regardless of the pool size, gave comparable and often superior classification performance to stool microscopy for the same number of tests. The urine pooling strategy with a pool size of 4 reduced the number of tests and total cost compared to classical stool microscopy.
Conclusions/significance: This study introduces a method for rapid and efficient S. mansoni prevalence estimation through examining pooled urine samples with POC-CCA as an alternative to widely used stool microscopy.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- WHO (2006) Preventive chemotherapy in human helminthiasis: coordinated use of anthelminthic drugs in control interventions: a manual for health professionals and programme managers. Geneva: World Health Organization.
-
- WHO (2011) Helminth control in school-age children: a guide for managers of control programmes. Geneva: World Health Organization.
-
- WHO (2012) Accelerating work to overcome the global impact of neglected tropical diseases: a roadmap for implementation. Geneva: World Health Organization.
-
- Lamberton PH, Kabatereine NB, Oguttu DW, Fenwick A, Webster JP (2014) Sensitivity and specificity of multiple Kato-Katz thick smears and a circulating cathodic antigen test for Schistosoma mansoni diagnosis pre- and post-repeated-praziquantel treatment. PLoS Negl Trop Dis. 8: e3139 10.1371/journal.pntd.0003139 . - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
