

Glycemic Control and the Risk of Tuberculosis: A Cohort Study
- PMID: 27505150
- PMCID: PMC4978445
- DOI: 10.1371/journal.pmed.1002072
Glycemic Control and the Risk of Tuberculosis: A Cohort Study
Abstract
Background: Diabetes is a well-known risk factor for tuberculosis (TB) and is increasingly prevalent in low- and middle-income countries, where the burden of TB is high. Glycemic control has the potential to modify the risk of TB. However, there are few studies on the association between glycemic control and TB risk, and the results are inconsistent.
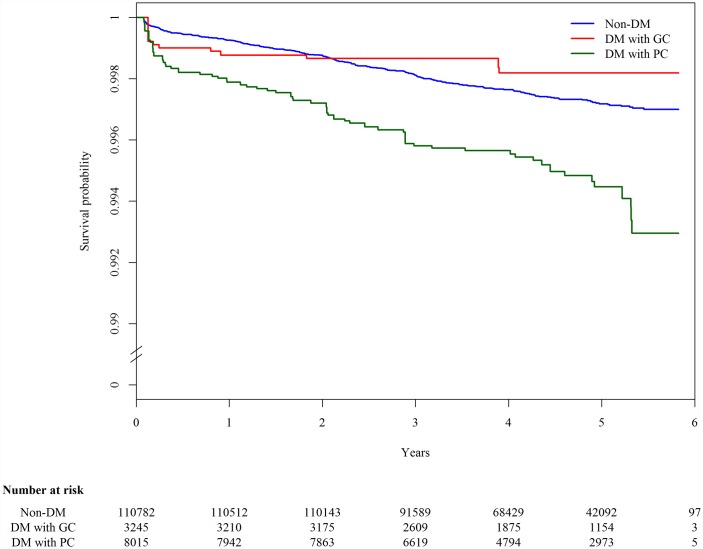
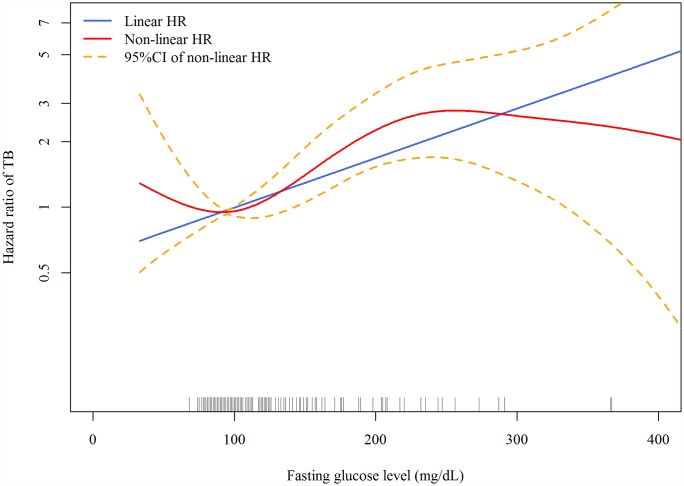
Methods and findings: We assembled a cohort using 123,546 individuals who participated in a community-based health screening service in northern Taiwan from 5 March 2005 to 27 July 2008. Glycemic control was measured using fasting plasma glucose (FPG) at the time of screening. The cohort was followed up to 31 December 2012 for the occurrence of TB by cross-matching the screening database to the national health insurance database. Multiple imputation was used to handle missing information. During a median follow-up of 4.6 y, 327 cases of TB occurred. In the multivariable Cox regression model, diabetic patients with poor glycemic control (FPG > 130 mg/dl) had a significantly higher hazard of TB (adjusted hazard ratio [aHR] 2.21, 95% CI 1.63-2.99, p < 0.001) compared to those without diabetes. The hazard of TB in diabetic patients with good glycemic control (FPG ≤ 130 mg/dl) did not differ significantly from that in nondiabetic individuals (aHR 0.69, 95% CI 0.35-1.36, p = 0.281). In the linear dose-response analysis, the hazard of TB increased with FPG (aHR 1.06 per 10-mg/dl increase in FPG, 95% CI 1.03-1.08, p < 0.001). Assuming the observed association between glycemic control and TB was causal, an estimated 7.5% (95% CI 4.1%-11.5%) of incident TB in the study population could be attributed to poor glycemic control. Limitations of the study include one-time measurement of fasting glucose at baseline and voluntary participation in the health screening service.
Conclusions: Good glycemic control could potentially modify the risk of TB among diabetic patients and may contribute to the control of TB in settings where diabetes and TB are prevalent.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization. Global strategy and targets for tuberculosis prevention, care and control after 2015. 2013 Nov 29 [cited 13 May 2015]. http://apps.who.int/gb/ebwha/pdf_files/EB134/B134_12-en.pdf?ua=1.
-
- Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek CJ, et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2.7 million participants. Lancet. 2011;378:31–40. 10.1016/S0140-6736(11)60679-X - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
