

Procedural Sedation Outside of the Operating Room Using Ketamine in 22,645 Children: A Report From the Pediatric Sedation Research Consortium
- PMID: 27505716
- PMCID: PMC5138082
- DOI: 10.1097/PCC.0000000000000920
Procedural Sedation Outside of the Operating Room Using Ketamine in 22,645 Children: A Report From the Pediatric Sedation Research Consortium
Abstract
Objective: Most studies of ketamine administered to children for procedural sedation are limited to emergency department use. The objective of this study was to describe the practice of ketamine procedural sedation outside of the operating room and identify risk factors for adverse events.
Design: Observational cohort review of data prospectively collected from 2007 to 2015 from the multicenter Pediatric Sedation Research Consortium.
Setting: Sedation services from academic, community, free-standing children's hospitals and pediatric wards within general hospitals.
Patients: Children from birth to 21 years old or younger.
Interventions: None.
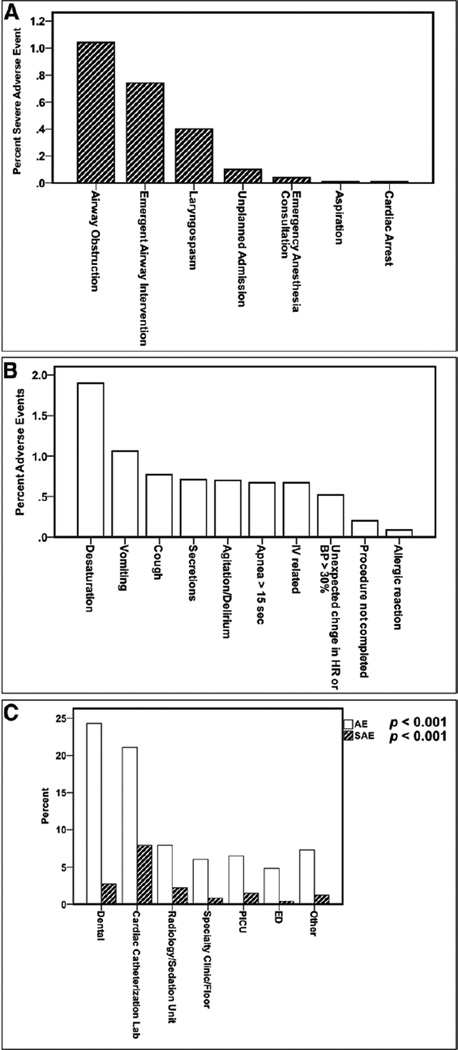
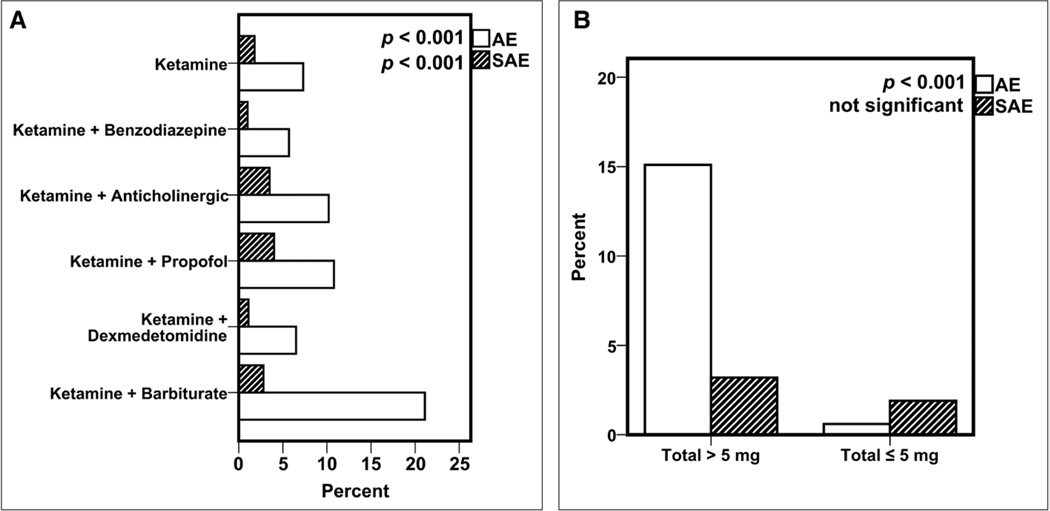
Measurements and main results: Describe patient characteristics, procedure type, and location of administration of ketamine procedural sedation. Analyze sedation-related adverse events and severe adverse events. Identify risk factors for adverse events using multivariable logistic regression. A total of 22,645 sedations performed using ketamine were analyzed. Median age was 60 months (range, < 1 mo to < 22 yr); 72.0% were American Society of Anesthesiologists-Physical Status less than III. The majority of sedations were performed in dedicated sedation or radiology units (64.6%). Anticholinergics, benzodiazepines, or propofol were coadministered in 19.8%, 57.9%, and 35.4%, respectively. The overall adverse event occurrence rate was 7.26% (95% CI, 6.92-7.60%), and the frequency of severe adverse events was 1.77% (95% CI, 1.60-1.94%). Procedures were not completed in 39 of 19,747 patients (0.2%). Three patients experienced cardiac arrest without death, all associated with laryngospasm.
Conclusions: This is a description of a large prospectively collected dataset of pediatric ketamine administration predominantly outside of the operating room. The overall incidence of severe adverse events was low. Risk factors associated with increased odds of adverse events were as follows: cardiac and gastrointestinal disease, lower respiratory tract infection, and the coadministration of propofol and anticholinergics.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Ketamine Again Outside the Operating Room? Yes It Works.Pediatr Crit Care Med. 2016 Dec;17(12):1179-1180. doi: 10.1097/PCC.0000000000000951. Pediatr Crit Care Med. 2016. PMID: 27918386 No abstract available.
References
-
- Petrack EM, Marx CM, Wright MS. Intramuscular ketamine is superior to meperidine, promethazine, and chlorpromazine for pediatric emergency department sedation. Arch Pediatr Adolesc Med. 1996;150:676–681. - PubMed
-
- Peña BM, Krauss B. Adverse events of procedural sedation and analgesia in a pediatric emergency department. Ann Emerg Med. 1999;34:483–491. - PubMed
-
- Ip U, Saincher A. Safety of pediatric procedural sedation in a Canadian emergency department. CJEM. 2000;2:15–20. - PubMed
-
- Roback MG, Wathen JE, MacKenzie T, et al. A randomized, controlled trial of i.v. versus i.m. ketamine for sedation of pediatric patients receiving emergency department orthopedic procedures. Ann Emerg Med. 2006;48:605–612. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
